
Safety Profile of COVID-19 Vaccines among Healthcare Workers in Poland

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
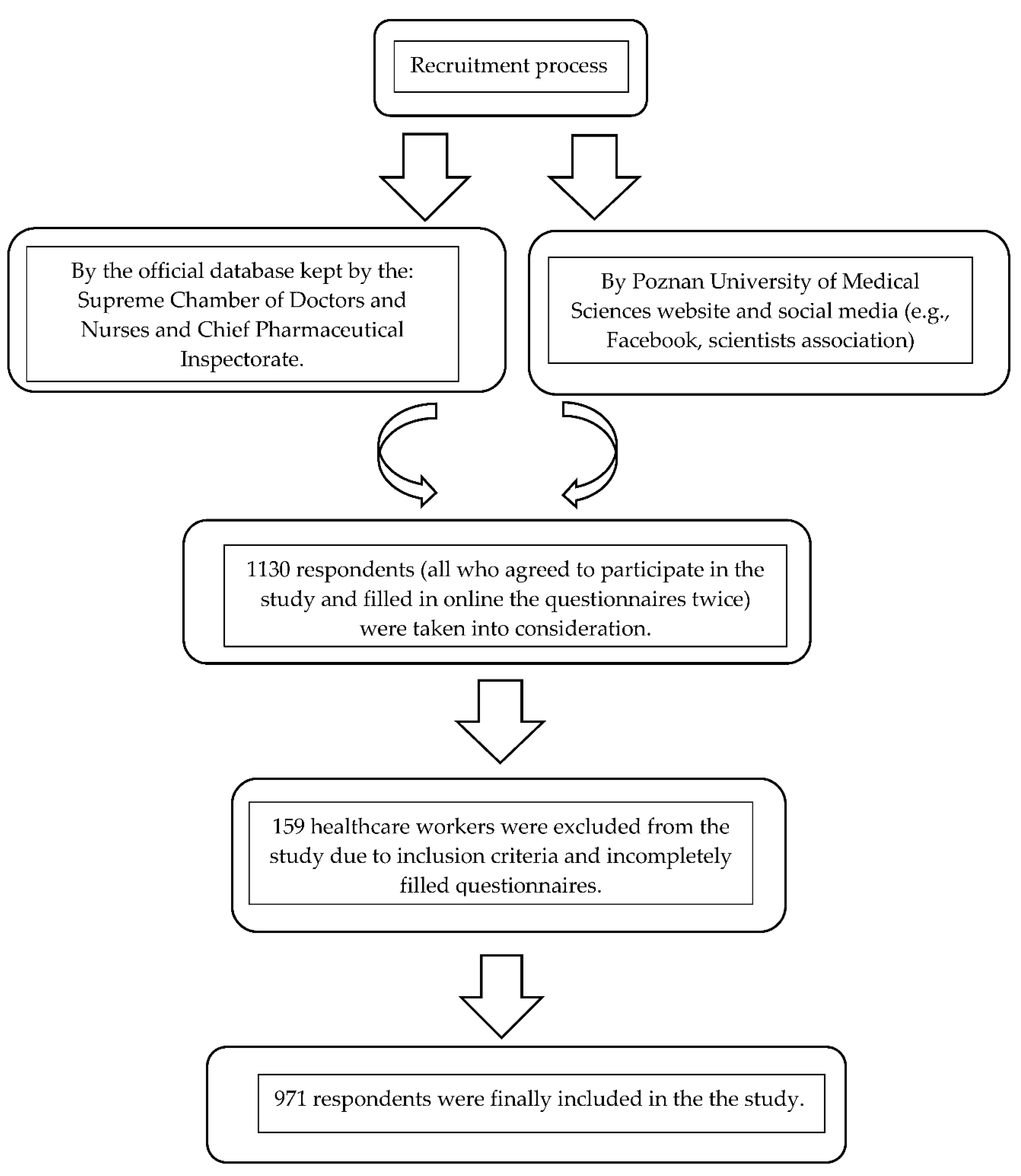
2.1. Study Population
- Group 1 (n = 676): Respondents vaccinated with two doses of vaccine BNT162b2 (Pfizer–BioNTech) against SARS-CoV-2 virus;
- Group 2 (n = 150): Respondents vaccinated with two doses of vaccine mRNA-1273 (Moderna) against SARS-CoV-2 virus;
- Group 3 (n = 145): Respondents vaccinated with two doses of vaccine ChAdOx1 nCoV-19 (Oxford–AstraZeneca) against SARS-CoV-2 virus.
2.2. Study Technique
- Demographic data (age, sex, height, weight, profession, and geographic region).
- Medical anamneses (chronic illnesses, health status, smoking, and alcohol consumption).
- COVID-19-related anamneses (type of vaccine, number of vaccine doses, dates of vaccine doses, previous infection, and diagnosis date).
- Vaccine side effects (local side effects, systemic side effects, onset, and duration).
2.3. Statistical Analysis
3. Results
3.1. Study Group Characteristics
3.2. Safety Profile of COVID-19 Vaccines
3.3. Identification of Sociodemographic and Clinical Factors Influencing the Risk of Side Effects Following the Intake of SARS-CoV-2 Virus Vaccines
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malik, Y.S.; Sircar, S.; Bhat, S.; Sharun, K.; Dhama, K.; Dadar, M.; Tiwari, R.; Chaicumpa, W. Emerging Novel Coronavirus (2019-Ncov)—Current Scenario, Evolutionary Perspective Based on Genome Analysis and Recent Developments. Vet. Q. 2020, 40, 68–76. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int (accessed on 15 January 2022).
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Dey, S.K. Efficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 4149. [Google Scholar] [CrossRef] [PubMed]
- Sacharczuk, W.; Dankowski, R.; Marciniak, A.; Szałek-Goralewska, A.; Szyszka, A. Cardiovascular Imaging in the Acute Phase of Coronavirus Disease 2019 (COVID-19). J. Med. Sci. 2021, 90, e532. [Google Scholar] [CrossRef]
- Seostianin, M.; Neumann-Podczaska, A.; Wieczorowska-Tobis, K. Towards effective collaboration of physicians and pharmacists for the care of older people (including COVID-19 perspective). J. Med. Sci. 2020, 89, e424. [Google Scholar] [CrossRef]
- Pormohammad, A.; Zarei, M.; Ghorbani, S.; Mohammadi, M.; Razizadeh, M.; Turner, D.; Turner, R. Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Vaccines 2021, 9, 467. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Mao, Q.; Zhang, J.; Bian, L.; Gao, F.; Wang, J.; Xu, M.; Liang, Z. COVID-19 Vaccines: Current Understanding on Immunogenicity, Safety, and Further Considerations. Front. Immunol. 2021, 12, 669339. [Google Scholar] [CrossRef] [PubMed]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing COVID-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Sharma, O.; Sultan, A.A.; Ding, H.; Triggle, C.R. A Review of the Progress and Challenges of Developing a Vaccine for COVID-19. Front. Immunol. 2020, 11, 585354. [Google Scholar] [CrossRef] [PubMed]
- Yuan, P.; Ai, P.; Liu, Y.; Ai, Z.; Wang, Y.; Cao, W.; Xia, X.; Zheng, J.C. Safety, Tolerability, and immunogenicity of COVID-19 vaccines: A systematic review and meta-analysis. medRxiv 2022. [Google Scholar] [CrossRef]
- Yan, Z.P.; Yang, M.; Lai, C.L. COVID-19 vaccines: A review of the safety and efficacy of current clinical trials. Pharmaceuticals 2021, 14, 406. [Google Scholar] [CrossRef] [PubMed]
- Krause, P.; Fleming, T.R.; Longini, I.; Henao-Restrepo, A.M.; Peto, R.; Dean, N.; Halloran, M.; Huang, Y.; Gilbert, P.; DeGruttola, V.; et al. COVID-19 vaccine trials should seek worthwhile efficacy. Lancet 2020, 396, 741–743. [Google Scholar] [CrossRef]
- Wu, Q.; Dudley, M.Z.; Chen, X.; Bai, X.; Dong, K.; Zhuang, T.; Salmon, D.; Yu, H. Evaluation of the safety profile of COVID-19 vaccines: A rapid review. BMC Med. 2021, 19, 173. [Google Scholar] [CrossRef] [PubMed]
- Serwis Rzeczypospolitej Polskiej. The National Vaccination Program. Available online: https://www.gov.pl/web/szczepimysie/narodowy-program-szczepien-przeciw-covid-19 (accessed on 15 September 2021).
- Riad, A.; Schünemann, H.; Attia, S.; Peričić, T.P.; Žuljević, M.F.; Jürisson, M.; Kalda, R.; Lang, K.; Morankar, S.; Yesuf, E.A.; et al. COVID-19 Vaccines Safety Tracking (CoVaST): Protocol of a Multi-Center Prospective Cohort Study for Active Surveillance of COVID-19 Vaccines’ Side Effects. Int. J. Environ. Res. Public Health 2021, 18, 7859. [Google Scholar] [CrossRef]
- Fal, A.F. COVID-19 Disease Characteristics, Symptoms and Health Effects. Recommendations and Experiences of Polish Clinicians. Science against the Pandemic. 2021. Available online: https://naukaprzeciwpandemii.pl/ (accessed on 4 February 2022).
- World Health Organization. Strategic Advisory Group of Experts on Immunization. WHO SAGE Roadmap for Prioritizing Uses of COVID-19 Vaccines in the Context of Limited Supply. November 2020. Available online: https://www.who.int/publications/i/item/who-sage-roadmap-for-prioritizing-uses-of-covid-19-vaccines-in-the-context-of-limited-supply (accessed on 15 January 2022).
- Characteristics of the Medicinal Product: Nuvaxovid Dispersion for Injection COVID-19 Vaccine (Recombinant, Adjuvanted). Available online: https://www.ema.europa.eu/en/documents/product-information/nuvaxovid-epar-product-information_pl.pdf (accessed on 15 January 2022).
- COVID-19 Vaccination Report in Poland. January 2022. Available online: https://www.gov.pl/web/szczepimysie/raport-szczepien-przeciwko-covid-19 (accessed on 15 January 2022).
- Hernandez, A.F.; Calina, D.; Poulas, K.; Docea, A.O.; Tsatsakis, A.M. Safety of COVID-19 vaccines administered in the EU: Should we be concerned? Toxicol. Rep. 2021, 8, 871–879. [Google Scholar] [CrossRef]
- COVID-19 Vaccines Safety Update. 20 January 2022. Available online: https://www.ema.europa.eu/en/documents/covid-19-vaccine-safety-update/covid-19-vaccines-safety-update-20-january-2022_en.pdf (accessed on 15 January 2022).
- Dziedzic, A.; Riad, A.; Attia, S.; Klugar, M.; Tanasiewicz, M. Self-Reported Adverse Events of COVID-19 Vaccines in Polish Healthcare Workers and Medical Students. Cross-Sectional Study and Pooled Analysis of CoVaST Project Results in Central Europe. J. Clin. Med. 2021, 10, 5338. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Alhazmi, A.; Alamer, E.; Dawas, D.; Hakami, M.; Darraj, M.; Abdelwahab, S.; Maghfuri, A.; Algaissi, A. Evaluation of Side Effects Associated with COVID-19 Vaccines in Saudi Arabia. Vaccines 2021, 9, 674. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 Vaccine Side Effects among Healthcare Workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Hocková, B.; Kantorová, L.; Slávik, R.; Spurná, L.; Stebel, A.; Havril’ak, M.; Klugar, M. Side Effects of mRNA-Based COVID-19 Vaccine: Nationwide Phase IV Study among Healthcare Workers in Slovakia. Pharmaceuticals 2021, 14, 873. [Google Scholar] [CrossRef] [PubMed]
- Funk, C.D.; Laferrière, C.; Ardakani, A. Target product profile analysis of COVID-19 vaccines in Phase III clinical trials and beyond: An early 2021 perspective. Viruses 2021, 13, 418. [Google Scholar] [CrossRef] [PubMed]
- Kounis, N.G.; Koniari, I.; de Gregorio, C.; Velissaris, D.; Petalas, K.; Brinia, A.; Assimakopoulos, S.F.; Gogos, C.; Kouni, S.N.; Kounis, G.N.; et al. Allergic Reactions to Current Available COVID-19 Vaccinations: Pathophysiology, Causality, and Therapeutic Considerations. Vaccines 2021, 9, 221. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 vaccine in a nationwide mass vaccination setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Daniel, W.; Nivet, M.; Warner, J.; Podolsky, D.K. Early Evidence of the Effect of SARS-CoV-2 Vaccine at One Medical Center. N. Engl. J. Med. 2021, 384, 1962–1963. [Google Scholar] [CrossRef] [PubMed]
- Ghazy, R.M.; Ashmawy, R.; Hamdy, N.A.; Elhadi, Y.A.M.; Reyad, O.A.; Elmalawany, D.; Almaghraby, A.; Shaaban, R.; Taha, S.H.N. Efficacy and Effectiveness of SARS-CoV-2 Vaccines: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 350. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID-19 Vaccine Effectiveness Research. Available online: https://www.cdc.gov/vaccines/covid-19/effectiveness-research/protocols.html (accessed on 15 January 2022).
- Gee, J.; Marquez, P.; Su, J.; Calvert, G.M.; Liu, R.; Myers, T.; Nair, N.; Martin, S.; Clark, T.; Markowitz, L.; et al. First Month of COVID-19 Vaccine Safety Monitoring—United States, December 14, 2020-January 13, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 283–288. [Google Scholar] [CrossRef] [PubMed]
- McNeil, M.M.; DeStefano, F. Vaccine-associated hypersensitivity. J. Allergy Clin. Immunol. 2018, 141, 463–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimabukuro, T.T.; Cole, M.; Su, J.R. Reports of anaphylaxis after receipt of mRNA COVID-19 vaccines in the US-December 14, 2020-January 18, 2021. JAMA 2021, 325, 1101–1102. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Davis, K.; Douoguih, M. Thrombotic thrombocytopenia after Ad26. COV2.S vaccination—Response from the manufacturer. N. Engl. J. Med. 2021, 384, 1965–1966. [Google Scholar] [CrossRef] [PubMed]
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and thrombocytopenia after ChAdOx1 nCoV-19 vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef] [PubMed]
- See, I.; Su, J.R.; Lale, A.; Woo, E.J.; Guh, A.Y.; Shimabukuro, T.T.; Streiff, M.B.; Rao, A.K.; Wheeler, A.P.; Beavers, S.F.; et al. US case reports of cerebral venous sinus thrombosis with thrombocytopenia after Ad26. COV2.S vaccination, March 2 to April 21, 2021. JAMA 2021, 325, 2448–2456. [Google Scholar] [CrossRef] [PubMed]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T.; et al. Preliminary findings of mRNA COVID-19 vaccine safety in pregnant persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.; Krauthammer, S.H.; Wolf, I.; Even-Sapir, E. Hypermetabolic lymphadenopathy following administration of BNT162b2 mRNA COVID-19 vaccine: Incidence assessed by [18F]FDG PET-CT and relevance to study interpretation. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1854–1863. [Google Scholar] [CrossRef] [PubMed]
- Frater, J.; Ewer, K.J.; Ogbe, A.; Pace, M.; Adele, S.; Adland, E.; Alagaratnam, J.; Aley, P.K.; Ali, M.; Ansari, M.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 in HIV infection: A singlearm substudy of a phase 2/3 clinical trial. Lancet HIV 2021, 8, e474–e485. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Type of SARS-CoV-2 Virus Vaccine | p Value | ||
|---|---|---|---|---|
| BNT162b2 (Group 1) | mRNA-1273 (Group 2) | ChAdOx1 nCoV-19 (Group 3) | ||
| Group size n (%) | 676 (69.62%) | 150 (15.45%) | 145 (14.93%) | |
| Gender (%): | 0.99153 * | |||
| Women | 78.25 | 78.00 | 78.62 | |
| Men | 21.75 | 22.00 | 21.38 | |
| Age (Mean ± SD) | 33.41 ± 14.77 | 34.74 ± 14.03 | 36.32 ± 15.08 | 0.06781 # |
| Self-estimated health status (%): | 0.18675 * | |||
| Excellent | 11.83 | 10.67 | 6.21 | |
| Very good | 50.44 | 49.33 | 48.28 | |
| Good | 34.02 | 34.00 | 38.62 | |
| Not so good | 3.25 | 4.67 | 6.90 | |
| Poor | 0.44 | 1.33 | 0.00 | |
| Presence of comorbidities (%) | 46.01 | 39.33 | 46.21 | 0.31541 * |
| Most common comorbidity types (%): | ||||
| Spine diseases | 5.47 a | 7.33 a | 11.03 b | 0.04605 * |
| Heart failure | 1.92 | 2.00 | 2.76 | 0.81208 * |
| Obesity | 5.18 | 9.33 | 4.83 | 0.12380 * |
| Hashimoto’s disease | 3.25 | 3.33 | 1.38 | 0.46709 * |
| Hypothyroidism | 7.25 a | 9.33 a | 2.07 b | 0.03243 * |
| Depression | 2.07 | 4.00 | 2.76 | 0.37660 * |
| Allergy | 16.27 | 13.33 | 15.86 | 0.67027 * |
| Arterial Hypertension | 9.76 a | 4.67 b | 13.10 a | 0.04212 * |
| Diabetes | 4.44 | 3.33 | 2.76 | 0.58041 * |
| Respiratory system diseases | 3.11 | 1.33 | 3.45 | 0.45559 * |
| Previous infection with SARS-CoV-2 virus (%) | 10.06 | 7.33 | 15.17 | 0.07648 * |
| Use of stimulants (%): | ||||
| Alcohol | 41.42 | 44.00 | 33.10 | 0.11724 * |
| Nicotine | 13.31 | 14.00 | 12.41 | 0.92193 * |
| Type of Side Effects (%) | Type of SARS-CoV-2 Virus Vaccine | p Value | |||
|---|---|---|---|---|---|
| BNT162b2 (Group 1) | mRNA-1273 (Group 2) | ChAdOx1 nCoV-19 (Group 3) | |||
| General | 53.11 a | 72.00 b | 67.59 b | <0.00001 * | |
| Local SE Prevalence | Pain at the injection site | 49.93 a | 69.33 b | 53.10 a | 0.00009 * |
| Swelling at the injection site | 8.47 a | 19.33 b | 3.45 a | <0.00001 * | |
| Systemic SE Prevalence | Headache | 28.89 a | 50.00 b | 42.76 b | <0.00001 * |
| Muscle pain | 25.00 a | 43.33 b | 46.90 b | <0.00001 * | |
| Chills | 19.67 a | 39.33 b | 46.21 b | <0.00001 * | |
| Fatigue | 30.18 | 39.33 | 33.10 | 0.08993 * | |
| Shortness of Breath | 0.15 | 0.67 | 0.00 | 0.37552 * | |
| Problems with concentration | 0.30 | 1.33 | 0.69 | 0.26254 * | |
| Joint pain | 9.20 a | 14.67 b | 24.14 c | <0.00001 * | |
| Fever | 16.57 a | 42.67 b | 51.72 b | <0.00001 * | |
| Dizziness | 0.30 a | 2.00 b | 1.38 b | 0.04945 * | |
| Nausea | 2.51 a | 10.67 b | 11.72 b | <0.00001 * | |
| Lymphadenopathy | 4.88 a | 14.00 b | 2.07 a | <0.00001 * | |
| Diarrhea | 0.30 a | 0.00 a | 2.07 b | 0.01620 * | |
| Insomnia | 0.44 | 0.67 | 1.38 | 0.42562 * | |
| Sweating | 0.15 | 0.00 | 0.69 | 0.35510 * | |
| Anaphylaxis | 0.00 | 0.00 | 0.00 | N/A | |
| Thrombosis | 0.00 | 0.00 | 0.00 | N/A | |
| Thrombocytopenia | 0.00 | 0.00 | 0.00 | N/A | |
| Skin-related SE Prevalence | Rash | 2.22 | 4.00 | 0.00 | 0.06056 * |
| Variable | Type of SARS-CoV-2 Virus Vaccine | p Value | ||
|---|---|---|---|---|
| BNT162b2 (Group 1) | mRNA-1273 (Group 2) | ChAdOx1 nCoV-19 (Group 3) | ||
| Vaccine dose followed by side effects (%): | <0.0001 * | |||
| 1 dose | 26.32 a | 28.70 a | 96.94 b | |
| 2 dose | 30.75 a | 25.00 a | 0.00 b | |
| 1 dose and 2 dose | 42.94 a | 46.30 a | 3.06 b | |
| Time the side effects started to appear (%): | 0.52475 * | |||
| 1 day after vaccination | 84.17 | 90.74 | 86.73 | |
| 2 days after vaccination | 12.78 | 8.33 | 13.27 | |
| 3 days after vaccination | 1.39 | 0.00 | 0.00 | |
| 4 days after vaccination | 1.11 | 0.00 | 0.00 | |
| 5 days after vaccination | 0.28 | 0.00 | 0.00 | |
| 6 days after vaccination | 0.28 | 0.93 | 0.00 | |
| Duration of side effects (days) (Mean ± SD &) | 2.53 ± 3.09 | 2.31 ± 1.39 | 2.40 ± 2.84 | 0.6647 # |
| Nature of the intensity of side effects (%): | <0.0001 * | |||
| mild | 37.40 a | 16.67 b | 20.41 b | |
| moderate | 55.68 a | 71.30 b | 66.33 b | |
| severe | 6.93 a | 12.04 b | 13.27 b | |
| Variable | Type of SARS-CoV-2 Virus Vaccine | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| BNT162b2 (Group 1) | mRNA-1273 (Group 2) | ChAdOx1 nCoV-19 (Group 3) | |||||||
| Confirmed SARS-CoV-2 Infection at Baseline | Confirmed SARS-CoV-2 Infection at Baseline | Confirmed SARS-CoV-2 Infection at Baseline | |||||||
| Yes | No | p Value | Yes | No | p Value | Yes | No | p Value | |
| Number of side effects (Mean ± SD) | 6.3 ± 3.2 | 5.6 ± 3.8 | 0.2823 * | 5.9 ± 4.2 | 6.3 ± 3.8 | 0.7269 * | 5.6 ± 3.3 | 6.2 ± 3.5 | 0.5807 * |
| Duration of side effects (days) (Mean ± SD) | 4.8 ± 3.0 | 4.0 ± 3.1 | 0.0364 * | 8.3 ± 2.5 | 5.7 ± 3.4 | 0.0052 * | 4.6 ± 3.4 | 5.7 ± 3.4 | 0.1994 * |
| Nature of the intensity of side effects n (%): | |||||||||
| mild | 18 (40.0) | 117 (37.0) | 1 (9.1) | 17 (17.5) | 0.278 # | 4 (30.8) | 16 (18.8) | 0.551 # | |
| moderate | 23 (51.1) | 178 (56.3) | 0.751 # | 10 (90.9) | 67 (69.1) | 8 (61.5) | 57 (67.1) | ||
| severe | 4 (8.9) | 21 (6.7) | 0 (0.0) | 13 (13.4) | 1 (7.7) | 12 (14.1) | |||
| Risk of Side Effects | ||||||
|---|---|---|---|---|---|---|
| BNT162b2 (Group 1) | mRNA-1273 (Group 2) | ChAdOx1-S (Group 3) | ||||
| Variable | Coeff. (95% CI) | p Value | Coeff. (95% CI) | p Value | Coeff. (95% CI) | p Value |
| Gender: | ||||||
| Female ref. | ||||||
| Male | 0.47 (0.32, 0.69) | <0.0001 | 0.42 (0.18, 0.96) | 0.040 | 0.83 (0.36, 1.93) | 0.681 |
| Age | 0.99 (0.97, 1.00) | 0.056 | 0.96 (0.94, 0.99) | 0.007 | 0.93 (0.90, 0.96) | <0.0001 |
| Self-estimated health status: | ||||||
| Excellent ref. | ||||||
| Very good | 0.62 (0.37, 1.01) | 0.058 | 2.41 (0.50, 11.63) | 0.271 | 0.74 (0.16, 3.28) | 0.697 |
| Good | 1.19 (0.85, 1.66) | 0.310 | 0.75 (0.34, 1.66) | 0.486 | 0.72 (0.33, 1.55) | 0.410 |
| Not so good | 1.27 (0.53, 3.06) | 0.585 | 0.46 (0.09, 2.24) | 0.338 | 0.24 (0.06, 0.55) | 0.086 |
| Poor | 1.13 (0.91, 1.39) | 0.256 | 2.89 (1.21, 2.41) | 0.516 | 1.22 (0.89, 1.66) | 0.309 |
| Most common comorbidity types: | ||||||
| Hashimoto’s disease | 2.41 (0.93, 6.25) | 0.069 | 1.57 (0.17, 14.53) | 0.688 | 0.47 (0.02, 7.75) | 0.601 |
| Allergy | 1.84 (1.20, 2.82) | 0.005 | 1.65 (0.51, 5.26) | 0.396 | 6.13 (1.37, 27.39) | 0.017 |
| Obesity | 1.05 (0.53, 2.08) | 0.886 | 1.47, 0.39, 5.57) | 0.567 | 2.99 (0.35, 25.66) | 25.66 |
| Heart failure | 1.03 (0.34, 3.09) | 0.957 | 0.77 (0.06, 8.76) | 0.836 | 0.46 (0.06, 3.43) | 0.456 |
| Diabetes | 0.87 (0.42, 1.82) | 0.727 | 1.57 (0.17, 14.53) | 0.688 | 0.15 (0.01, 1.49) | 0.106 |
| Hypothyroidism | 1.56 (0.86, 2.86) | 0.142 | 1.47 (0.39, 5.57) | 0.567 | 0.95 (0.08, 10.84) | 0.973 |
| Respiratory system diseases | 2.91 (1.05, 8.03) | 0.039 | 0.88 (0.51, 1.96) | 0.866 | 1.95 (0.21, 18.01) | 0.553 |
| Spine diseases | 1.06 (0.73, 1.89) | 0.856 | 1.57 (0.87, 2.66) | 0.155 | 1.86 (0.99, 2.01) | 0.884 |
| Use of stimulants: | ||||||
| Alcohol | 1.05 (0.77, 1.43) | 0.719 | 1.06 (0.51, 2.19) | 0.860 | 1.08 (0.51, 2.27) | 0.833 |
| Nicotine | 0.70 (0.45, 1.10) | 0.124 | 0.96 (0.34, 2.68) | 0.950 | 0.25 (0.09, 0.70) | 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paczkowska, A.; Hoffmann, K.; Michalak, M.; Hans-Wytrychowska, A.; Bryl, W.; Kopciuch, D.; Zaprutko, T.; Ratajczak, P.; Nowakowska, E.; Kus, K. Safety Profile of COVID-19 Vaccines among Healthcare Workers in Poland. Vaccines 2022, 10, 434. https://doi.org/10.3390/vaccines10030434
Paczkowska A, Hoffmann K, Michalak M, Hans-Wytrychowska A, Bryl W, Kopciuch D, Zaprutko T, Ratajczak P, Nowakowska E, Kus K. Safety Profile of COVID-19 Vaccines among Healthcare Workers in Poland. Vaccines. 2022; 10(3):434. https://doi.org/10.3390/vaccines10030434
Chicago/Turabian StylePaczkowska, Anna, Karolina Hoffmann, Michał Michalak, Anna Hans-Wytrychowska, Wiesław Bryl, Dorota Kopciuch, Tomasz Zaprutko, Piotr Ratajczak, Elżbieta Nowakowska, and Krzysztof Kus. 2022. "Safety Profile of COVID-19 Vaccines among Healthcare Workers in Poland" Vaccines 10, no. 3: 434. https://doi.org/10.3390/vaccines10030434