
Myocardial Injury as a Prognostic Factor in Mid- and Long-Term Follow-Up of COVID-19 Survivors


 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
3. Results
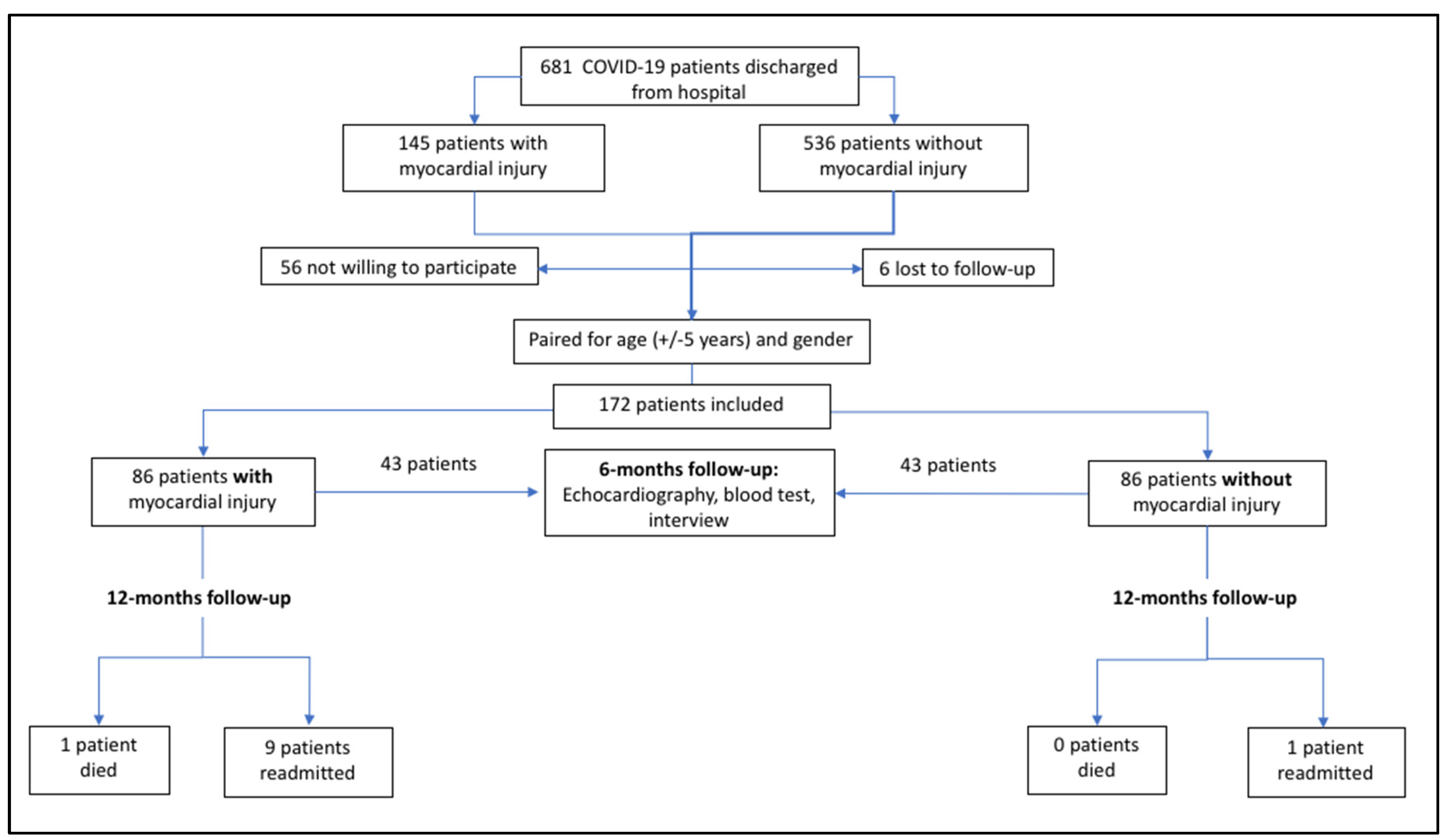
3.1. Patients
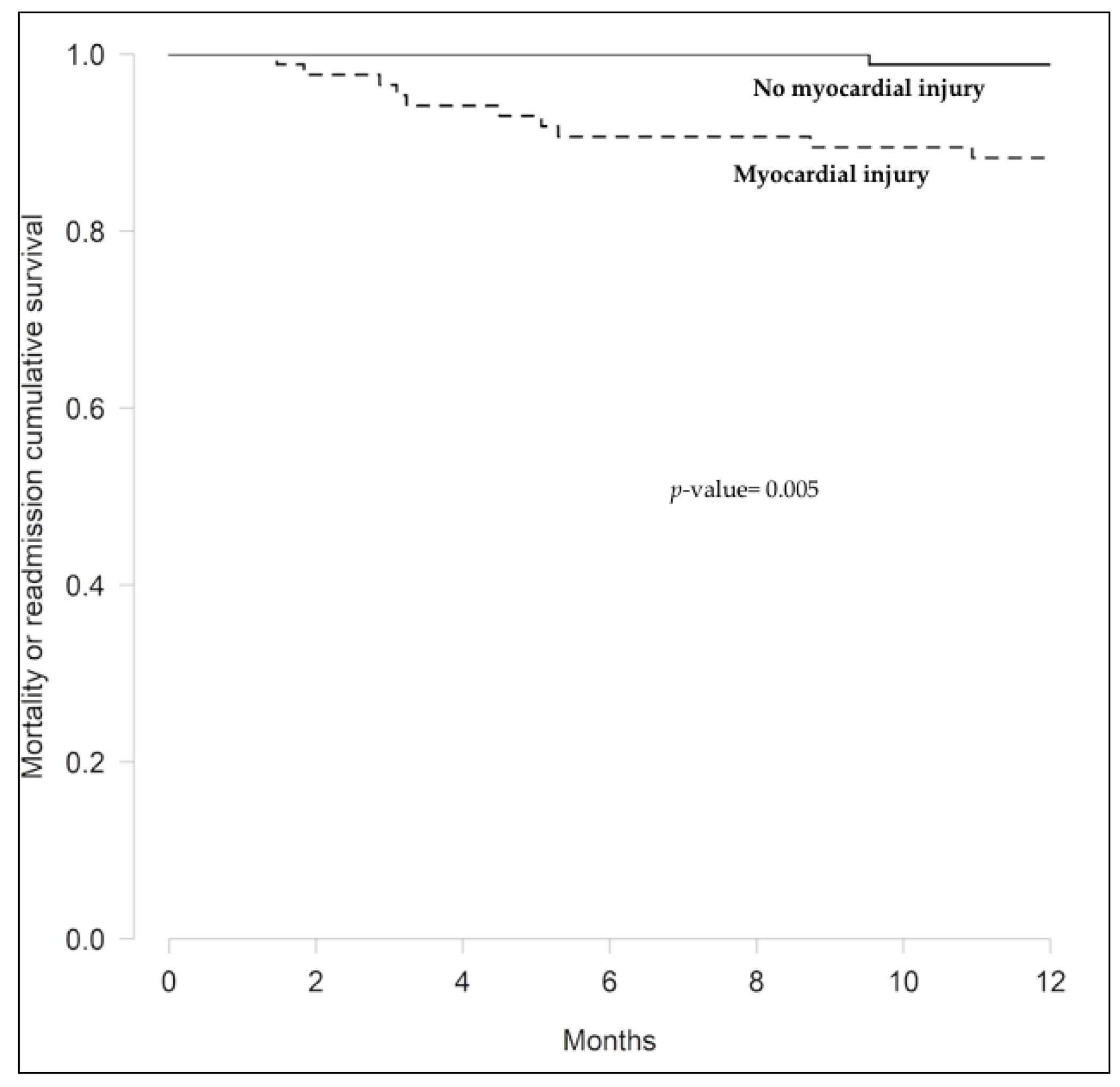
3.2. Myocardial Injury and Long-Term Prognosis
3.3. Echocardiographic, Laboratory and Clinical Characteristics at Six Months
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- COVID-19 Clinical Management: Living Guidance. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-clinical-2021-1 (accessed on 6 November 2021).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, transmission, and pathogenesis of SARS-CoV-2. BMJ 2020, 371, m3862. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y.; Dong, W. Clinical sequelae of COVID-19 survivors in Wuhan, China: A single-centre longitudinal study. Clin. Microbiol. Infect. 2021, 27, 89–95. [Google Scholar] [CrossRef]
- Negreira-Caamaño, M.; Martínez-Del Río, J.; Águila-Gordo, D.; Mateo-Gómez, C.; Soto-Pérez, M.; Piqueras-Flores, J. Cardio-Vascular Events after COVID-19 Hospitalization: Long-Term Folow-Up. Available online: http://www.revespcardiol.org/en-cardiovascular-events-after-COVI-19-hospitalization-avance-S0300893221003225 (accessed on 11 November 2021).
- Zhao, Y.-M.; Shang, Y.-M.; Song, W.-B.; Li, Q.-Q.; Xie, H.; Xu, Q.-F.; Jia, J.-L.; Li, L.-M.; Mao, H.-L.; Zhou, X.-M.; et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine 2020, 25, 100463. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, T.; Knight, D.S.; Razvi, Y.; Kumar, K.; Vimalesvaran, K.; Thornton, G.; Patel, R.; Chacko, L.; Brown, J.T.; Coyle, C.; et al. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur. Heart J. 2021, 42, 1866–1878. [Google Scholar] [CrossRef] [PubMed]
- Kini, A.; Cao, D.; Nardin, M.; Sartori, S.; Zhang, Z.; Pivato, C.A.; Chiarito, M.; Nicolas, J.; Vengrenyuk, Y.; Krishnamoorthy, P.; et al. Types of myocardial injury and mid-term outcomes in patients with COVID-19. Eur. Heart J. -Qual. Care Clin. Outcomes 2021, 7, 438–446. [Google Scholar] [CrossRef]
- Zheng, Y.-Y.; Ma, Y.-T.; Zhang, J.-Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. Covid-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802. [Google Scholar] [CrossRef]
- Peiró, Ó.M.; Carrasquer, A.; Sánchez-Giménez, R.; Lal-Trehan, N.; Del-Moral-Ronda, V.; Bonet, G.; Fort-Gallifa, I.; Picó-Plana, E.; Bastón-Paz, N.; Gutiérrez, C.; et al. Biomarkers and short-term prognosis in COVID-19. Biomarkers 2021, 26, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Carrasquer, A.; Peiró, Ó.M.; Sánchez-Gímenez, K.; Lal-Trehan, N.; Del-Moral-Ronda, V.; Bardají, A. Implicaciones pronósticas del Índice de Charlson y el daño miocárdico en pacientes COVID-19 atendidos en urgencias. Emergencias 2021, 33, 481–483. [Google Scholar] [PubMed]
- Siripanthong, B.; Nazarian, S.; Muser, D.; Deo, R.; Santangeli, P.; Khanji, M.Y.; Cooper, L.T.; Chahal, C.A.A. Recognizing COVID-19–related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management. Heart Rhythm 2020, 17, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Akhmerov, A.; Marbán, E. COVID-19 and the Heart. Circ. Res. 2020, 126, 1443–1455. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.P.; Blet, A.; Smyth, D.; Li, H. The Science Underlying COVID-19. Circulation 2020, 142, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Vestjens, S.M.T.; Spoorenberg, S.M.C.; Rijkers, G.T.; Grutters, J.C.; Ten Berg, J.M.; Noordzij, P.G.; Van de Garde, E.; Bos, W. High-sensitivity cardiac troponin T predicts mortality after hospitalization for community-acquired pneumonia. Respirology 2017, 22, 1000–1006. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Long, D.A.; Tannenbaum, L.; Koyfman, A. An emergency medicine approach to troponin elevation due to causes other than occlusion myocardial infarction. Am. J. Emerg. Med. 2020, 38, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Fernández, A.; Izquierdo, A.; Subirana, I.; Farré, N.; Vila, J.; Durán, X.; García-Guimaraes, M.; Valdivielso, S.; Cabero, P.; Soler, C.; et al. Markers of myocardial injury in the prediction of short-term COVID-19 prognosis. Rev. Esp. Cardiol. 2021, 74, 576–583. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Salvatici, M.; Barbieri, B.; Cioffi, S.M.G.; Morenghi, E.; Leone, F.P.; Maura, F.; Moriello, G.; Sandri, M.T. Association between cardiac troponin I and mortality in patients with COVID-19. Biomarkers 2020, 25, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Stefanini, G.G.; Chiarito, M.; Ferrante, G.; Cannata, F.; Azzolini, E.; Viggiani, G.; De Marco, A.; Briani, M.; Bocciolone, M.; Bragato, R.; et al. Early detection of elevated cardiac biomarkers to optimise risk stratification in patients with COVID-19. Heart 2020, 106, 1512–1518. [Google Scholar] [CrossRef] [PubMed]
- Bardají, A.; Carrasquer, A.; Sánchez-Giménez, R.; Lal-Trehan, N.; Del-Moral-Ronda, R.; Peiró, Ó.M.; Bonet, G.; Castilho, G.; Fort-Gallifa, I.; Benavent, C.; et al. Prognostic implications of myocardial injury in patients with and without COVID-19 infection treated in a university hospital. Rev. Esp. Cardiol. 2021, 74, 24–32. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Tan, C.; Wu, J.; Chen, M.; Wang, Z.; Luo, L.; Zhou, X.; Liu, X.; Huang, X.; Yuan, S.; et al. Impact of coronavirus disease 2019 on pulmonary function in early convalescence phase. Respir. Res. 2020, 21, 1–10. [Google Scholar] [CrossRef]
- Liu, C.; Ye, L.; Xia, R.; Zheng, X.; Yuan, C.; Wang, Z.; Lin, R.; Shi, D.; Gao, Y.; Yao, J.; et al. Chest Computed Tomography and Clinical Follow-Up of Discharged Patients with COVID-19 in Wenzhou City, Zhejiang, China. Ann. Am. Thorac. Soc. 2020, 17, 1231–1237. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Babapoor-Farrokhran, S.; Gill, D.; Walker, J.; Rasekhi, R.T.; Bozorgnia, B.; Amanullah, A. Myocardial injury and COVID-19: Possible mechanisms. Life Sci. 2020, 253, 117723. [Google Scholar] [CrossRef]
- Guzik, T.J.; Mohiddin, S.A.; DiMarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F.M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D’Acquisto, F.; et al. COVID-19 and the cardiovascular system: Implications for risk assessment, diagnosis, and treatment options. Cardiovasc. Res. 2020, 116, 1666–1687. [Google Scholar] [CrossRef]
- Imazio, M.; Klingel, K.; Kindermann, I.; Brucato, A.; De Rosa, F.G.; Adler, Y.; De Ferrari, G.M. COVID-19 pandemic and troponin: Indirect myocardial injury, myocardial inflammation or myocarditis? Heart 2020, 106, 1127–1131. [Google Scholar] [CrossRef] [PubMed]
- Mueller, C.; Giannitsis, E.; Jaffe, A.S.; Huber, K.; Mair, J.; Cullen, L.; Hammarsten, O.; Mills, N.L.; Möckel, M.; Krychtiuk, K.; et al. Cardiovascular biomarkers in patients with COVID-19. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Jirak, P.; Larbig, R.; Shomanova, Z.; Fröb, E.J.; Dankl, D.; Torgersen, C.; Frank, N.; Mahringer, M.; Butkiene, D.; Haake, H.; et al. Myocardial injury in severe COVID-19 is similar to pneumonias of other origin: Results from a multicentre study. ESC Heart Fail. 2021, 8, 37–46. [Google Scholar] [CrossRef]
- Gao, C.; Wang, Y.; Gu, X.; Shen, X.; Zhou, D.; Zhou, S.; Huang, J.-A.; Cao, B.; Guo, Q. Association Between Cardiac Injury and Mortality in Hospitalized Patients Infected with Avian Influenza A (H7N9) Virus. Crit. Care Med. 2020, 48, 451–458. [Google Scholar] [CrossRef]
- Bois, M.C.; Boire, N.A.; Layman, A.J.; Aubry, M.-C.; Alexander, M.P.; Roden, A.C.; Hagen, C.E.; Quinton, R.A.; Larsen, C.; Erben, Y.; et al. COVID-19–Associated Nonocclusive Fibrin Microthrombi in the Heart. Circulation 2021, 143, 230–243. [Google Scholar] [CrossRef]
- Pellegrini, D.; Kawakami, R.; Guagliumi, G.; Sakamoto, A.; Kawai, K.; Gianatti, A.; Nasr, A.; Kutys, R.; Guo, L.; Cornelissen, A.; et al. Microthrombi as a Major Cause of Cardiac Injury in COVID-19. Circulation 2021, 143, 1031–1042. [Google Scholar] [CrossRef]
- Lombardi, C.M.; Carubelli, V.; Iorio, A.; Inciardi, R.M.; Bellasi, A.; Canale, C.; Camporotondo, R.; Catagnano, F.; Dalla Vecchia, L.A.; Giovinazzo, S.; et al. Association of Troponin Levels with Mortality in Italian Patients Hospitalized With Coronavirus Disease 2019: Results of a Multicenter Study. JAMA Cardiol. 2020, 5, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Qin, M.; Cai, Y.; Liu, T.; Shen, B.; Yang, F.; Cao, S.; Liu, X.; Xiang, Y.; Zhao, Q.; et al. Characteristics and clinical significance of myocardial injury in patients with severe coronavirus disease 2019. Eur. Heart J. 2020, 41, 2070–2079. [Google Scholar] [CrossRef]
- Bardají, A.; Cediel, G.; Carrasquer, A.; de Castro, R.; Sánchez, R.; Boqué, C. Troponin Elevation in Patients Without Acute Coronary Syndrome. Rev. Esp. Cardiol. 2015, 68, 469–476. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Myocardial Injury (n = 86) | No Myocardial Injury (n = 86) | p-Value | |
|---|---|---|---|
| Clinical characteristics | |||
| Age, years * | 70.5 (60–74) | 69.0 (60–74) | 0.692 |
| Women | 29.2% | 31.95% | 0.867 |
| Hypertension | 73.3% | 50.0% | 0.003 |
| Dyslipidaemia | 43.0% | 32.6% | 0.208 |
| Ever smoked | 29.6% | 29.8% | 1.00 |
| Diabetes mellitus | 30.2% | 17.6% | 0.080 |
| Chronic kidney disease | 10.5% | 2.35% | 0.064 |
| Chronic heart failure | 9.30% | 1.16% | 0.034 |
| Coronary heart disease | 10.5% | 8.14% | 0.793 |
| Atrial fibrillation | 12.8% | 4.76% | 0.115 |
| COPD | 11.6% | 10.5% | 1.00 |
| Cerebrovascular disease | 5.88% | 2.33% | 0.277 |
| Peripheral vascular disease | 4.65% | 4.65% | 1.00 |
| Laboratory analysis results | |||
| Leukocytes/µL×10 3 * | 7.63 (5.89–14.4) | 5.95 (5.26–9.14) | 0.115 |
| Lymphocytes/µL×103 * | 0.98 (0.68–1.73) | 1.25 (0.9–2.29) | 0.039 |
| Haemoglobin, g/dL ** | 13.1 (1.74) | 13.9 (1.74) | 0.008 |
| Creatinine, mg/dL * | 0.99 (0.79–1.3) | 0.84 (0.68–1.02) | 0.001 |
| LDH U/L * | 329 (270–449) | 279 (240–356) | 0.001 |
| C-reactive protein, mg/dL * | 10.0 (4.20–18.0) | 7.10 (3.90–11.9) | 0.020 |
| D-Dimer, ng/mL * | 950 (610–1920) | 600 (420–1150) | 0.002 |
| All Patients (n = 172) | Myocardial Injury (n = 86) | No Myocardial Injury (n = 86) | p-Value * | |
|---|---|---|---|---|
| Composite endpoint ** | 11 | 10 | 1 | 0.01 |
| Death | 1 | 1 | 0 | 1.00 |
| Hospital readmission | 0.02 | |||
| Total | 10 | 9 | 1 | |
| Cardiovascular cause | 4 | 3 | 1 | |
| Non-cardiovascular cause | 6 | 6 | 0 |
| Myocardial Injury (n = 43) | No Myocardial Injury (n = 43) | p-Value | |
|---|---|---|---|
| Echocardiographic characteristics | |||
| Interventricular septum wall thickness, mm * | 10.0 (9.00–12.0) | 9.00 (8.00–10.5) | 0.002 |
| Posterior wall thickness, mm * | 10.0 (9.00–11.0) | 8.00 (7.00–10.0) | 0.002 |
| LV telediastolic diameter, mm * | 50.0 (45.0–55.5) | 49.0 (45.0–53.0) | 0.659 |
| LV telesistolic diameter, mm * | 30.0 (26.5–34.5) | 30.0 (27.0–32.5) | 0.274 |
| LV end diastolic volume, mL * | 91.0 (81.0–108) | 85.0 (75.5–101) | 0.111 |
| LV end systolic volume, mL * | 33.0 (26.0–46.0) | 32.0 (25.0–41.5) | 0.380 |
| LV ejection fraction (Simpson’s biplane), % * | 63.0 (60.0–67.5) | 63.0 (58.0–67.8) | 0.833 |
| TAPSE, mm * | 23.0 (21.0–25.0) | 23.0 (20.2–24.8) | 0.951 |
| E/E’ratio * | 8.00 (6.2–9.50) | 8.00 (6.00–9.05) | 0.303 |
| PAP, mmHg * | 34.0 (27.5–37.8) | 29.0 (27.0–31.0) | 0.021 |
| Laboratory characteristics | |||
| Urea, mg/dL * | 43.0 (35.0–52.0) | 38.0 (32.5–44.6) | 0.028 |
| Creatinine, mg/dL * | 1.01 (0.88–1.17) | 0.91 (0.81–1.04) | 0.041 |
| Glomerular filtrate rate, mL/min/1.73 m2 ** | 71.5 (24.3) | 82.9 (20.4) | 0.021 |
| C-Reactive Protein, mg/dL * | 0.18 (0.10–0.37) | 0.13 (0.08–0.24) | 0.236 |
| NT-proBNP, pg/L * | 119 (73.9–234) | 71.3 (32.9–120) | 0.001 |
| Haemoglobin, g/dL ** | 13.2 (1.40) | 14.1 (1.29) | 0.002 |
| Leukocytes/µL×103 * | 7020 (6170–7790) | 6600 (5395–7670) | 0.260 |
| Lymphocytes/µL×103 * | 1910 (1235–2205) | 2080 (1710–2555) | 0.062 |
| D-Dimer, ng/mL * | 295 (205–388) | 230 (190–375) | 0.137 |
| Clinical characteristics | |||
| Chest pain | 4.65% | 2.33% | 1.00 |
| Palpitations | 4.65% | 0.00% | 0.494 |
| NYHA functional class I-II NYHA functional class III-IV | 93.0% 7.00% | 97.7% 2.30% | 0.407 |
| Pulse oximetry * | 98.0 (97.0–99.0) | 97.0 (96.5–98.0) | 0.098 |
| Systolic blood pressure ** | 141 (17.0) | 136 (18.6) | 0.194 |
| Diastolic blood pressure ** | 77.3 (11.7) | 77.9 (13.2) | 0.826 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izquierdo, A.; Mojón, D.; Bardají, A.; Carrasquer, A.; Calvo-Fernández, A.; Carreras-Mora, J.; Giralt, T.; Pérez-Fernández, S.; Farré, N.; Soler, C.; et al. Myocardial Injury as a Prognostic Factor in Mid- and Long-Term Follow-Up of COVID-19 Survivors. J. Clin. Med. 2021, 10, 5900. https://doi.org/10.3390/jcm10245900
Izquierdo A, Mojón D, Bardají A, Carrasquer A, Calvo-Fernández A, Carreras-Mora J, Giralt T, Pérez-Fernández S, Farré N, Soler C, et al. Myocardial Injury as a Prognostic Factor in Mid- and Long-Term Follow-Up of COVID-19 Survivors. Journal of Clinical Medicine. 2021; 10(24):5900. https://doi.org/10.3390/jcm10245900
Chicago/Turabian StyleIzquierdo, Andrea, Diana Mojón, Alfredo Bardají, Anna Carrasquer, Alicia Calvo-Fernández, José Carreras-Mora, Teresa Giralt, Sílvia Pérez-Fernández, Núria Farré, Cristina Soler, and et al. 2021. "Myocardial Injury as a Prognostic Factor in Mid- and Long-Term Follow-Up of COVID-19 Survivors" Journal of Clinical Medicine 10, no. 24: 5900. https://doi.org/10.3390/jcm10245900
APA StyleIzquierdo, A., Mojón, D., Bardají, A., Carrasquer, A., Calvo-Fernández, A., Carreras-Mora, J., Giralt, T., Pérez-Fernández, S., Farré, N., Soler, C., Solà-Richarte, C., Cabero, P., Vaquerizo, B., Marrugat, J., & Ribas, N. (2021). Myocardial Injury as a Prognostic Factor in Mid- and Long-Term Follow-Up of COVID-19 Survivors. Journal of Clinical Medicine, 10(24), 5900. https://doi.org/10.3390/jcm10245900