
Serological Response to SARS-CoV-2 in Health Care Workers Employed in a Large Tertiary Hospital in Lombardy, Northern Italy

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population, and Design
2.2. Laboratory Procedures
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
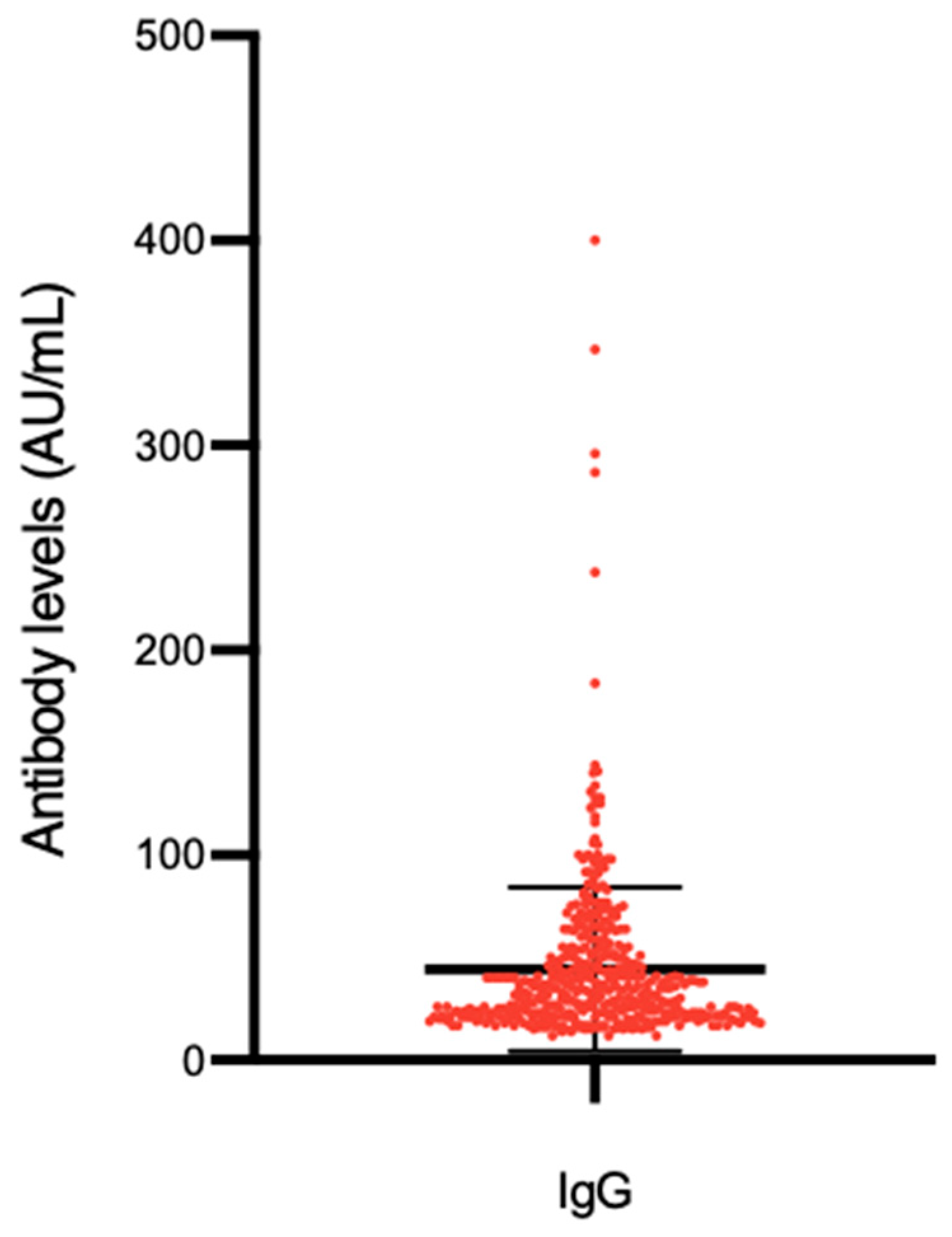
3.2. Seroprevalence of SARS-CoV-2 S1/S2 IgG Antibodies
3.3. Cumulative Prevalence of SARS-CoV-2 Infection
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Tabata, S.; Imai, K.; Kawano, S.; Ikeda, M.; Kodama, T.; Miyoshi, K.; Obinata, H.; Mimura, S.; Kodera, T.; Kitagaki, M.; et al. Clinical characteristics of COVID-19 in 104 people with SARS-CoV-2 infection on the Diamond Princess cruise ship: A retrospective analysis. Lancet Infect. Dis. 2020, 20, 1043–1050. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. Prevalence of Asymptomatic SARS-CoV-2 Infection. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.E.; Li, Z.; Chiew, C.J.; Yong, S.E.; Toh, M.P.; Lee, V.J. Presymptomatic Transmission of SARS-CoV-2-Singapore. Morb. Mortal Wkly Rep. 2020, 69, 411–415. [Google Scholar] [CrossRef] [Green Version]
- Long, Q.-X.; Liu, B.-Z.; Deng, H.-J.; Wu, G.-C.; Deng, K.; Chen, Y.-K.; Liao, P.; Qiu, J.-F.; Lin, Y.; Cai, X.-F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Xiang, F.; Wang, X.; He, X.; Peng, Z.; Yang, B.; Zhang, J.; Zhou, Q.; Ye, H.; Ma, Y.; Li, H.; et al. Antibody Detection and Dynamic Characteristics in Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 1930–1934. [Google Scholar] [CrossRef] [PubMed]
- Dati della Sorveglianza Integrata COVID-19 in Italia. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-dashboard (accessed on 29 November 2020).
- Piva, S.; Filippini, M.; Turla, F.; Cattaneo, S.; Margola, A.; De Fulviis, S.; Nardiello, I.; Beretta, A.; Ferrari, L.; Trotta, R.; et al. Clinical presentation and initial management critically ill patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in Brescia, Italy. J. Crit. Care 2020, 58, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Rizzi, M.; Castelli, F.; Latronico, N.; Focá, E. SARS-CoV-2 invades the West. How to face a COVID-19 epidemic in Lombardy, Northern Italy? Infez. Med. 2020, 28, 133–134. [Google Scholar]
- Iversen, K.; Bundgaard, H.; Hasselbalch, R.B.; Kristensen, J.H.; Nielsen, P.B.; Pries-Heje, M.; Knudsen, A.D.; Christensen, C.E.; Fogh, K.; Norsk, J.B.; et al. Risk of COVID-19 in health-care workers in Denmark: An observational cohort study. Lancet Infect. Dis. 2020, 2, 3–10. [Google Scholar]
- World Health Organization. Transmission of SARS-CoV-2: Implications for Infection Prevention Precautions. Available online: https://www.who.int/publications/i/item/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations (accessed on 29 November 2020).
- Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. Available online: https://www.cdc.gov/coronavirus/2019-nCoV/hcp/infection-control.html (accessed on 29 November 2020).
- Black, J.R.M.; Bailey, C.; Przewrocka, J.; Dijkstra, K.K.; Swanton, C. COVID-19: The case for health-care worker screening to prevent hospital transmission. Lancet 2020, 395, 1418–1420. [Google Scholar] [CrossRef]
- Steensels, D.; Oris, E.; Coninx, L.; Nuyens, D.; Delforge, M.-L.; Vermeersch, P.; Heylen, L. Hospital-Wide SARS-CoV-2 Antibody Screening in 3056 Staff in a Tertiary Center in Belgium. JAMA 2020, 324, 195. [Google Scholar] [CrossRef]
- Poulikakos, D.; Sinha, S.; Kalra, P.A. SARS-CoV-2 antibody screening in healthcare workers in a tertiary centre in North West England. J. Clin. Virol. 2020, 129, 104545. [Google Scholar] [CrossRef]
- Fusco, F.M.; Pisaturo, M.; Iodice, V.; Bellopede, R.; Tambaro, O.; Parrella, G.; Di Flumeri, G.; Viglietti, R.; Pisapia, R.; Carleo, M.A.; et al. COVID-19 among healthcare workers in a specialist infectious diseases setting in Naples, Southern Italy: Results of a cross-sectional surveillance study. J. Hosp. Infect. 2020, 105, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Stubblefield, W.B.; Talbot, H.K.; Feldstein, L.R.; Tenforde, M.W.; Rasheed, M.A.U.; Mills, L.; Lester, S.N.; Freeman, B.; Thornburg, N.J.; Jones, I.D.; et al. Seroprevalence of SARS-CoV-2 Among Frontline Healthcare Personnel during the First Month of Caring for Patients with COVID-19—Nashville, Tennessee. Clin. Infect. Dis. 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Tenforde, M.W.; Stubblefield, W.B.; Feldstein, L.R.; Steingrub, J.S.; Shapiro, N.I.; Ginde, A.S.; Prekker, M.E.; Brown, S.M.; Peltan, I.D.; et al. Seroprevalence of SARS-CoV-2 Among Frontline Health Care Personnel in a Multistate Hospital Network—13 Academic Medical Centers, April–June 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.J.; Wilmore, S.M.S.; McCann, N.S.; Donnelly, O.; Lai, R.W.L.; Kinsella, M.J.; Rochford, H.L.; Patel, T. Seroprevalence of SARS-CoV-2 antibodies in healthcare workers at a London NHS Trust. Infect. Control Hosp. Epidemiol. 2020, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Dilaghi, E.; Prestigiacomo, C.; Alessio, G.; Marcellini, L.; Simmaco, M.; Santino, I.; Orsi, G.B.; Anibaldi, P.; Marcolongo, A.; et al. Prevalence of Sars-Cov-2 infection in health workers (HWs) and diagnostic test performance: The experience of a teaching hospital in central Italy. Int. J. Environ. Res. Public Health 2020, 17, 4417. [Google Scholar] [CrossRef]
- Garcia-Basteiro, A.L.; Moncunill, G.; Tortajada, M.; Vidal, M.; Guinovart, C.; Jiménez, A.; Santano, R.; Sanz, S.; Méndez, S.; Llupià, A.; et al. Seroprevalence of antibodies against SARS-CoV-2 among health care workers in a large Spanish reference hospital. Nat. Commun. 2020, 11, 3500. [Google Scholar] [CrossRef]
- World Health Organization. Global Surveillance for COVID-19 Caused by Human Infection with COVID-19 Virus: Interim Guidance. 20 March 2020. Available online: https://apps.who.int/iris/handle/10665/331506 (accessed on 29 November 2020).
- Bonelli, F.; Sarasini, A.; Zierold, C.; Calleri, M.; Bonetti, A.; Vismara, C.; Blocki, F.; Pallavicini, L.; Chinali, A.; Campisi, D.; et al. Clinical and analytical performance of an automated serological test that identifies S1/S2-neutralizing igG in COVID-19 patients semiquantitatively. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef]
- Peres, D.; Monteiro, J.; Almeida, M.A.; Ladeira, R. Risk perception of COVID-19 among Portuguese healthcare professionals and the general population. J. Hosp. Infect. 2020, 105, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.B.; Grüter, L.; Boltzmann, M.; Rollnik, J.D. Prevalence of serum IgG antibodies against SARS-CoV-2 among clinic staff. PLoS ONE 2020, 15, e0235417. [Google Scholar] [CrossRef] [PubMed]
- Korth, J.; Wilde, B.; Dolff, S.; Anastasiou, O.E.; Krawczyk, A.; Jahn, M.; Cordes, S.; Ross, B.; Esser, S.; Lindemann, M.; et al. SARS-CoV-2-specific antibody detection in healthcare workers in Germany with direct contact to COVID-19 patients. J. Clin. Virol. 2020, 128, 104437. [Google Scholar] [CrossRef]
- ISTAT, Salute M della. Primi Risultati dell’indagine di Sieroprevalenza sul SARS-CoV-2. 2020, p. 10. Available online: https://www.istat.it/it/files//2020/08/ReportPrimiRisultatiIndagineSiero.pdf (accessed on 20 December 2020).
- Percivalle, E.; Cambiè, G.; Cassaniti, I.; Nepita, E.V.; Maserati, R.; Ferrari, A.; Di Martino, R.; Isernia, P.; Mojoli, F.; Bruno, R.; et al. Prevalence of SARS-CoV-2 specific neutralising antibodies in blood donors from the Lodi Red Zone in Lombardy, Italy, as at 06 April 2020. Eurosurveillance 2020, 25, 1–5. [Google Scholar] [CrossRef]
- Valenti, L.; Bergna, A.; Pelusi, S.; Facciotti, F.; Lai, A.; Tarkowski, M.; Berzuini, A.; Caprioli, F.; Santoro, L.; Baselli, G.; et al. SARS-CoV-2 seroprevalence trends in healthy blood donors during the COVID-19 Milan outbreak. medRxiv 2020, 1–18. [Google Scholar] [CrossRef]
- Fontanet, A.; Cauchemez, S. COVID-19 herd immunity: Where are we? Nat. Rev. Immunol. 2020, 20, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int. J. Emerg. Med. 2020, 13, 1–8. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19) Interim Guidelines for COVID-19 Antibody Testing Current Status of Antibody Testing in the United States Antigenic Targets. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html (accessed on 29 November 2020).




{kind=link}
{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Age, mean (std) | 44 (10.7) |
| Female, n (%) | 1459 (77.1) |
| Professional category, n (%) | |
| Physicians | 411 (21.7) |
| Nurses a | 818 (43.2) |
| Support staff | 272 (14.3) |
| Lab technician/Other technicians | 24 (1.3) |
| Psychologist. healthcare assistant | 20 (1.1) |
| Other health personnel b | 216 (11.4) |
| Pharmacists. employees | 132 (7) |
| Working in a COVID-19 unit/ER, n (%) | 1008 (53.2) |
| Comorbidities c, n (%) | 613 (32.4) |
| Pregnancy, n (%) | 22 (1.2) |
| Underlying immunosuppression, n (%) | 45 (2.4) |
| Close contact with confirmed COVID-19 case, n (%) | 1098 (58) |
| Close contact with suspected COVID-19 case, n (%) | 736 (38.9) |
| Reporting COVID-19 compatible symptoms, n (%) | 922 (48.7) |
| Previously diagnosed with positive SARS-CoV-2 rt-PCR, n (%) | 290 (22.4) d |
| Hospitalization among symptomatic subject, n (%) | 24/922 (2.6) |
| Medical ward | 20/922 (2.2) |
| ICU | 4/922 (0.4) |
| Radiologic evidence of viral pneumonia, n (%) | 48/112 e (42.9) |
| Oxygen therapy, n (%) | 28/922 (3) |
| Variables | Serological Test | OR (95% CI) | p Value | |
|---|---|---|---|---|
| Positive Ab (n = 433) | Negative Ab (n = 1460) | |||
| Age, mean (std) | 45 (11) | 44 (11) | 0.013c | |
| Female, n (%) | 330 (76.2) | 1129 (77.3) | 0,9 (0.7;1.2) | 0.6 d |
| Working in a COVID-19 unit/ER, n (%) | 234 (54) | 774 (53) | 1.04 (0.8; 1.3) | 0.7 d |
| Comorbidities, n (%) | 141 (32.6) | 472 (32.3) | 1 (0.8; 1.3) | 0.9 d |
| Pregnancy, n (%) | 7 (1.6) | 15 (1) | 1.6 (0.6; 3.9) | 0.3 d |
| Underlying immunosuppression, n (%) | 12 (2.8) | 33 (2.3) | 1.2 (0.6; 2.4) | 0.6 d |
| Chronic steroid therapy, n (%) | 4 (0.9) | 18 (1.2) | 0.7 (0.2; 2.2) | 0.8 d |
| Other immunosuppressive therapy, n (%) | 7 (1.6) | 14 (1) | 1.7 (0.7; 4.2) | 0.3 d |
| COVID-19 compatible signs/symptoms, n (%) | 377 (87) | 545 (37.3) | 11.3 (8.4; 15.2) | <0.0001d |
| Duration of signs and symptoms (in days), mean (std) | 25 (24) | 20 (21) | 0.001c | |
| Delay time between signs and symptoms onset and serology test (in days), mean (std) | 48 (14) | 49 (18) | 0.3 c | |
| Previously diagnosed with positive SARS-CoV-2 RT-PCR a, n (%) | 248 (61) | 42 (4.7) | 10.1 (6.7; 15.2) | <0.0001d |
| Radiologic evidence of viral pneumonia b, n (%) | 46 (12.2) | 2 (0.37) | 37.7 (9; 156.4) | <0.0001d |
| Oxygen therapy b, n (%) | 17 (4.5) | 1 (0.2) | 25 (3.4; 193) | <0.0001d |
| Hydroxychloroquine treatment, n (%) | 63 (14.5) | 23 (1.6) | 10.6 (6.5; 17.4) | <0.0001d |
| Close contact with confirmed COVID-19 case, n (%) | 284 (65.6) | 814 (55.7) | 1.5 (1.2; 1.9) | <0.0001d |
| Close contact with suspected COVID-19 case, n (%) | 231 (53.4) | 505 (34.6) | 2.2 (1.7; 2.7) | <0.0001d |
| Serological Test | OR (95% CI) | p-Value | ||
|---|---|---|---|---|
| Negative Ab | Positive Ab | |||
| COVID-19 compatible symptoms | 545 | 377 | 11.3 (8.4; 15.2) | <0.0001 |
| Fever, n (%) | 167 (30.6) | 234 (62) | 3.7 (2.8; 4.8) | <0.0001 |
| Fatigue, n (%) | 341 (62.6) | 314 (83.3) | 3 (2.2; 4.1) | <0.0001 |
| Headache, n (%) | 278 (51) | 214 (56.8) | 1.3 (0.9; 1.6) | 0.09 |
| Myalgia, n (%) | 215 (39.4) | 245 (65) | 2.9 (2.2; 3.7) | <0.0001 |
| Cough, n (%) | 175 (31.1) | 183 (48.5) | 2 (1.5; 2.6) | <0.0001 |
| Dyspnea, n (%) | 70 (12.8) | 124 (32.8) | 3.3 (2.4; 4.6) | <0.0001 |
| Anosmia, n (%) | 47 (8.6) | 218 (57.8) | 14.5 (10.1; 20.8) | <0.0001 |
| Ageusia, n (%) | 59 (10.8) | 212 (56.2) | 10.6 (7.5; 14.8) | <0.0001 |
| Conjunctivitis, n (%) | 73 (13.4) | 42 (11.1) | 0.8 (0.5; 1.2) | 0.4 |
| Rhinitis, n (%) | 162 (29.7) | 117 (31) | 1.1 (0.8; 1.4) | 0.7 |
| Gastrointestinal discomfort, n (%) | 157 (28.8) | 149 (39.5) | 1.6 (1.2; 2.1) | 0.001 |
| Dermatological lesions, n (%) | 18 (3.3) | 30 (8) | 2.5 (1.4; 4.6) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comelli, A.; Focà, E.; Sansone, E.; Tomasi, C.; Albini, E.; Quiros-Roldan, E.; Tomasoni, L.R.; Sala, E.; Bonfanti, C.; Caccuri, F.; et al. Serological Response to SARS-CoV-2 in Health Care Workers Employed in a Large Tertiary Hospital in Lombardy, Northern Italy. Microorganisms 2021, 9, 488. https://doi.org/10.3390/microorganisms9030488
Comelli A, Focà E, Sansone E, Tomasi C, Albini E, Quiros-Roldan E, Tomasoni LR, Sala E, Bonfanti C, Caccuri F, et al. Serological Response to SARS-CoV-2 in Health Care Workers Employed in a Large Tertiary Hospital in Lombardy, Northern Italy. Microorganisms. 2021; 9(3):488. https://doi.org/10.3390/microorganisms9030488
Chicago/Turabian StyleComelli, Agnese, Emanuele Focà, Emanuele Sansone, Cesare Tomasi, Elisa Albini, Eugenia Quiros-Roldan, Lina Rachele Tomasoni, Emma Sala, Carlo Bonfanti, Francesca Caccuri, and et al. 2021. "Serological Response to SARS-CoV-2 in Health Care Workers Employed in a Large Tertiary Hospital in Lombardy, Northern Italy" Microorganisms 9, no. 3: 488. https://doi.org/10.3390/microorganisms9030488