

Do Comorbidities and Daily Medication before SARS-CoV-2 Infection Play a Role in Self-Reported Post-Infection Symptoms?
Abstract
:1. Introduction
2. Materials and Methods
Statistics
3. Results
3.1. Study Cohort
3.2. Comorbidities and Medication Prior to SARS-CoV-2 Infection
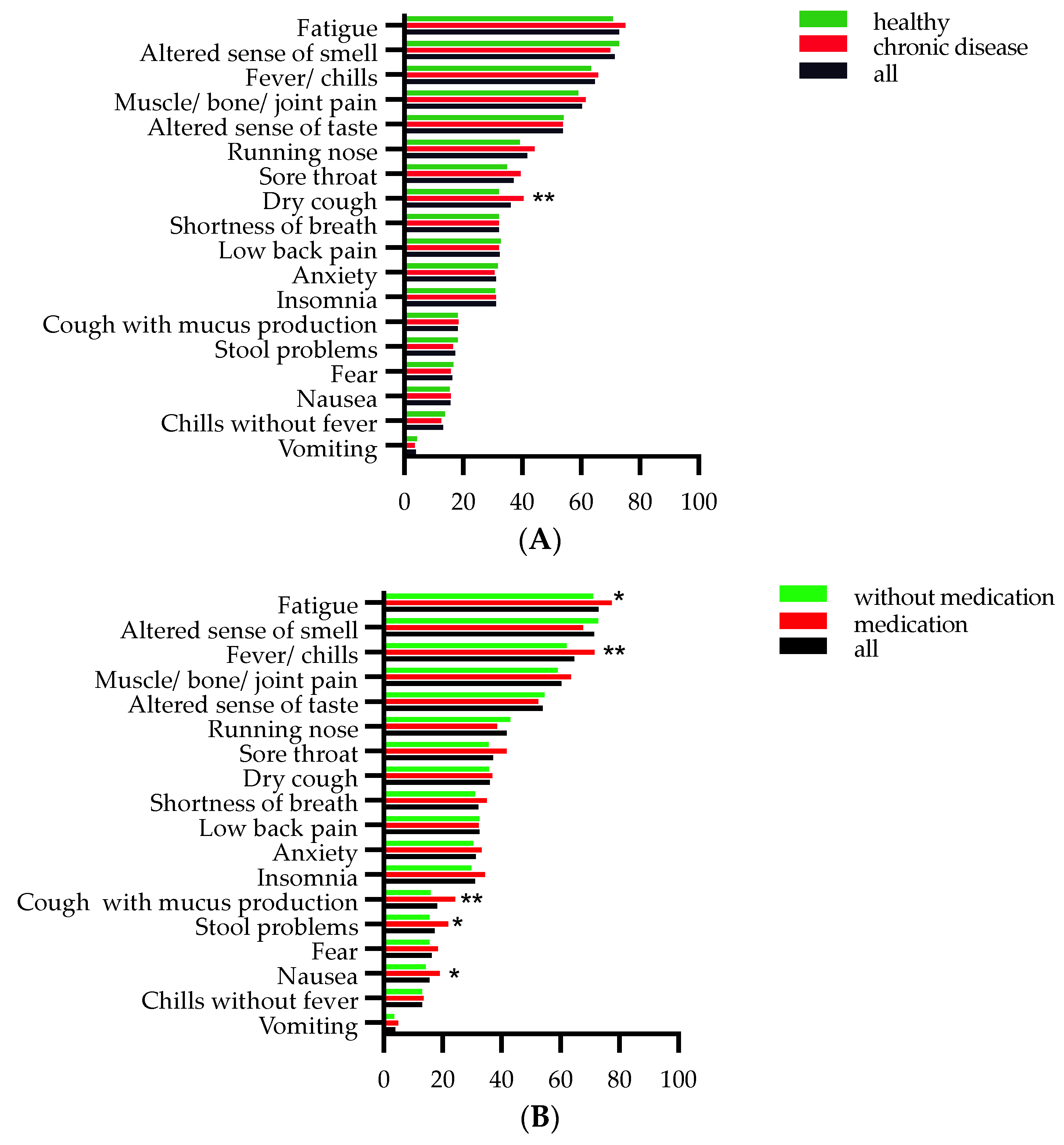
3.3. Associations between Comorbidities, Daily Medications, and Acute Symptoms
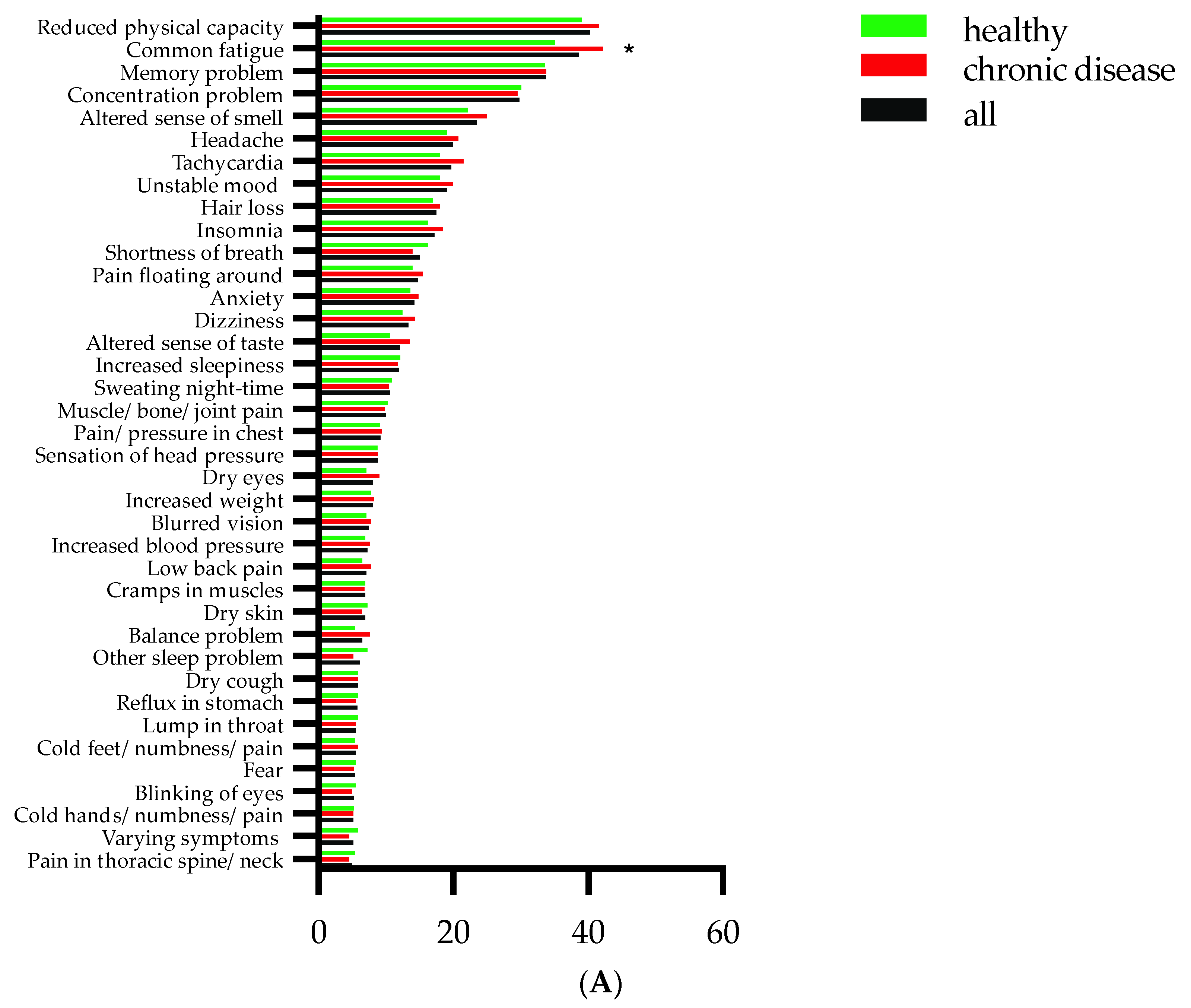
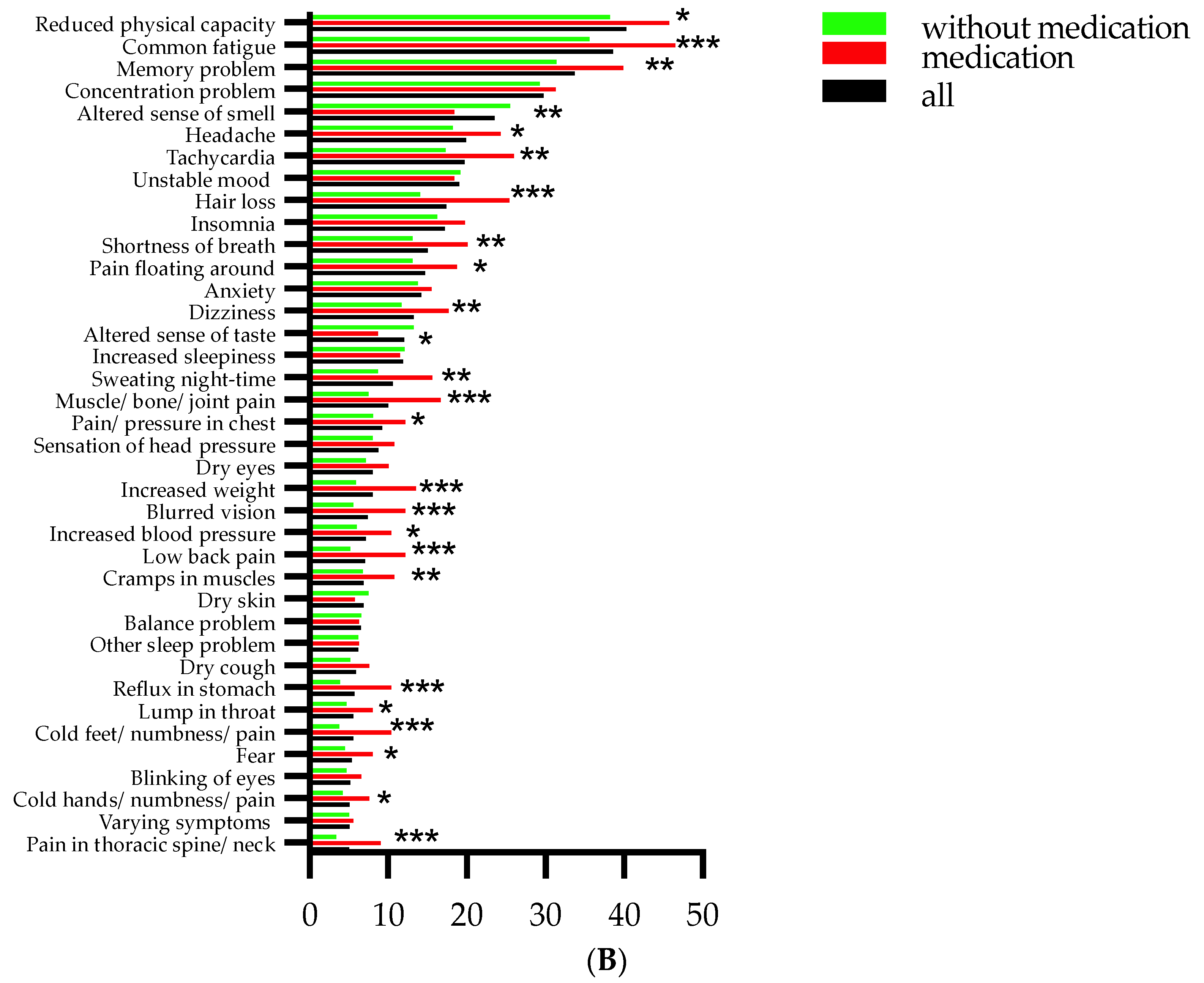
3.4. Associations between Comorbidities, Medication, and Persistent Symptoms
3.5. Regression Analysis for Predictors of Persistent Symptoms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 6 October 2021).
- Whitaker, M.; Elliott, J.; Chadeau-Hyam, M.; Riley, S.; Darzi, A.; Cooke, G.; Ward, H.; Elliott, P. Persistent COVID-19 symptoms in a community study of 606,434 people in England. Nat. Commun. 2022, 13, 1957. [Google Scholar] [CrossRef] [PubMed]
- Pavli, A.; Theodoridou, M.; Maltezou, H.C. Post-COVID Syndrome: Incidence, Clinical Spectrum, and Challenges for Primary Healthcare Professionals. Arch. Med. Res. 2021, 52, 575–581. [Google Scholar] [CrossRef]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; Jarvis, H.C.; et al. ‘Long-COVID’: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2021, 76, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.J.; Williams, D.M.; Walker, A.J.; Mitchell, R.E.; Niedzwiedz, C.L.; Yang, T.C.; Huggins, C.F.; Kwong, A.S.F.; Silverwood, R.J.; Di Gessa, G.; et al. Long COVID burden and risk factors in 10 UK longitudinal studies and electronic health records. Nat. Commun. 2022, 13, 3528. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef]
- Gasmi, A.; Peana, M.; Pivina, L.; Srinath, S.; Gasmi Benahmed, A.; Semenova, Y.; Menzel, A.; Dadar, M.; Bjorklund, G. Interrelations between COVID-19 and other disorders. Clin. Immunol. 2021, 224, 108651. [Google Scholar] [CrossRef]
- Li, J.; He, X.; Yuan, Y.; Zhang, W.; Li, X.; Zhang, Y.; Li, S.; Guan, C.; Gao, Z.; Dong, G. Meta-analysis investigating the relationship between clinical features, outcomes, and severity of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia. Am. J. Infect. Control 2021, 49, 82–89. [Google Scholar] [CrossRef]
- Yin, T.; Li, Y.; Ying, Y.; Luo, Z. Prevalence of comorbidity in Chinese patients with COVID-19: Systematic review and meta-analysis of risk factors. BMC Infect. Dis. 2021, 21, 200. [Google Scholar] [CrossRef]
- Kayaaslan, B.; Eser, F.; Kalem, A.K.; Kaya, G.; Kaplan, B.; Kacar, D.; Hasanoglu, I.; Coskun, B.; Guner, R. Post-COVID syndrome: A single-center questionnaire study on 1007 participants recovered from COVID-19. J. Med. Virol. 2021, 93, 6566–6574. [Google Scholar] [CrossRef]
- Moreno-Perez, O.; Merino, E.; Leon-Ramirez, J.M.; Andres, M.; Ramos, J.M.; Arenas-Jimenez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Norrefalk, J.R.; Borg, K.; Bileviciute-Ljungar, I. Self-scored impairments in functioning and disability in post-COVID syndrome following mild COVID-19 infection. J. Rehabil. Med. 2021, 53, jrm00239. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Yang, J.; Zhao, F.; Zhi, L.; Wang, X.; Liu, L.; Bi, Z.; Zhao, Y. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin. Res. Cardiol. 2020, 109, 531–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, P.T.; Garcia, P.D.; Salas, M.R.; Sanchez, R.R.; Avendano-Ortiz, J.; Guerrero-Monjo, S.; Garcia, F.; Llamas, M.A.; Lopez-Collazo, E.; Saz-Leal, P.; et al. SARS-CoV-2 IgG seropositivity in a cohort of 449 non-hospitalized individuals during Spanish COVID-19 lockdown. Sci. Rep. 2021, 11, 21612. [Google Scholar] [CrossRef]
- Xie, Y.; Bowe, B.; Al-Aly, Z. Burdens of post-acute sequelae of COVID-19 by severity of acute infection, demographics and health status. Nat. Commun. 2021, 12, 6571. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized COVID-19 “long haulers”. Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef]
- Soraas, A.; Bo, R.; Kalleberg, K.T.; Stoer, N.C.; Ellingjord-Dale, M.; Landro, N.I. Self-reported Memory Problems 8 Months After COVID-19 Infection. JAMA Netw. Open 2021, 4, e2118717. [Google Scholar] [CrossRef]
- Becker, J.H.; Lin, J.J.; Doernberg, M.; Stone, K.; Navis, A.; Festa, J.R.; Wisnivesky, J.P. Assessment of Cognitive Function in Patients After COVID-19 Infection. JAMA Netw. Open 2021, 4, e2130645. [Google Scholar] [CrossRef]
- Augustin, M.; Schommers, P.; Stecher, M.; Dewald, F.; Gieselmann, L.; Gruell, H.; Horn, C.; Vanshylla, K.; Cristanziano, V.D.; Osebold, L.; et al. Post-COVID syndrome in non-hospitalised patients with COVID-19: A longitudinal prospective cohort study. Lancet Reg. Health Eur. 2021, 6, 100122. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-de-Las-Penas, C.; Martin-Guerrero, J.D.; Pellicer-Valero, O.J.; Navarro-Pardo, E.; Gomez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalon, J.A.; Cigaran-Mendez, M.; Hernandez-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J. Clin. Med. 2022, 11, 413. [Google Scholar] [CrossRef] [PubMed]
- Bliddal, S.; Banasik, K.; Pedersen, O.B.; Nissen, J.; Cantwell, L.; Schwinn, M.; Tulstrup, M.; Westergaard, D.; Ullum, H.; Brunak, S.; et al. Acute and persistent symptoms in non-hospitalized PCR-confirmed COVID-19 patients. Sci. Rep. 2021, 11, 13153. [Google Scholar] [CrossRef] [PubMed]
- Soraas, A.; Kalleberg, K.T.; Dahl, J.A.; Soraas, C.L.; Myklebust, T.A.; Axelsen, E.; Lind, A.; Baevre-Jensen, R.; Jorgensen, S.B.; Istre, M.S.; et al. Persisting symptoms three to eight months after non-hospitalized COVID-19, a prospective cohort study. PLoS ONE 2021, 16, e0256142. [Google Scholar] [CrossRef]
- COVID-19 Lietuvoje (COVID-19 in Lithuania). COVID-19 amžiaus grupių dinamika. Available online: https://mpiktas.github.io/covid19lt/agegroups.html (accessed on 31 May 2021).




{kind=link}
{kind=link}
{kind=link}
| Total, n = 1050 | With Persistent Symptoms n = 812 | Without Persistent Symptoms n = 238 | ||
|---|---|---|---|---|
| Gender | Female | 927 (88.3%) | 719 (88.5%) | 208 (87.4%) |
| Male | 123 (11.7%) | 93 (11.5%) | 30 (12.6%) | |
| Age group | Younger than 40 years | 520 (49.5%) | 405 (49.9%) | 115 (48.3%) |
| 41–60 years | 475 (45.2%) | 370 (45.6%) | 105 (44.1%) | |
| 61–80 years | 55 (5.2%) | 37 (4.6%) | 18 (7.6%) | |
| Education | Primary/secondary | 134 (12.8%) | 102 (12.5%) | 32 (13.5%) |
| Higher non-university | 327 (31.1) | 252 (31%) | 75 (31.5%) | |
| Higher university | 589 (56.1%) | 458 (56.4%) | 131 (55%) | |
| Socioeconomic situation | Employed/working | 975 (92.9%) | 755 (93%) | 220 (92.4%) |
| Temporary unemployed | 23 (2.2%) | 17 (2.1%) | 6 (2.5%) | |
| Unemployed | 42 (4%) | 34 (4.2%) | 8 (3.4%) | |
| Retired | 9 (0.9%) | 5 (0.6%) | 4 (1.7%) | |
| Student | 1 (0.1%) | 1 (0.1%) | 0 |
| Disorders | Number of Participants | The Most Common Condition within Each Group |
|---|---|---|
| Cardiovascular | 194 (19%) | High blood pressure, n = 153 (15%) |
| Endocrine | 121 (12%) | Obesity, n = 96 (9%) |
| Thyroidea-related | 82 (8%) | Hypothyroidism, n = 53 (5%) |
| Neurological | 103 (10%) | Unspecified neurological diseases, excluding sleep disorders and epilepsy, n = 65 (6%) |
| Psychiatric | 74 (7%) | Anxiety, n = 55 (5%) |
| Gastrointestinal | 74 (7%) | Unspecified diseases of gastrointestinal tracts, n = 69 (7%) |
| Allergies | 71 (7%) | Unspecified allergic diseases, n = 71 (7%) |
| Pulmonary | 53 (5%) | Asthma, n = 34 (3%) |
| Inflammatory rheumatic | 34 (3%) | Unspecified rheumatic diseases, n = 33 (3%) |
| Chronic pain | 32 (3%) | Chronic pain syndrome, n = 25 (2%) |
| Haematological | 19 (2%) | Anaemia, n = 12 (1%) |
| Oncological | 18 (2%) | Unspecified oncological diseases, n = 18 (2%) |
| Dermatological | 18 (2%) | Unspecified skin diseases, n = 12 (1%) |
| Renal | 11 (1%) | Unspecified kidney diseases, n = 11 (1%) |
| Gynaecological | 10 (0.9%) | Unspecified gynaecological diseases, n = 8 (0.8%) |
| Immunodeficiency | 6 (0.6%) | Unspecified immunodeficiency diseases, n = 6 (0.6%) |
| Others: | 3 (0.3%) | Other 3 (0.3%) |
| Regressors | Crude OR (95% CI), p-Value | Adjusted OR (95% CI), p-Value |
|---|---|---|
| Medication before infection | 1.83 (1.28–2.62), <0.001 | 1.66 (1.10–2.44), 0.009 |
| Total comorbidities | 1.00 (0.9–1.11), 0.99 | 0.98 (0.9–1.1), 0.77 |
| Total number of acute symptoms | 1.40 (1.32–1.49), <0.001 | 1.40 (1.32–1.48), < 0.001 |
| Gender | 0.9 (0.58–1.39), 0.63 | 0.89 (0.55–1.43), 0.6 |
| Age | 1.0 (0.99–1.0), 0.75 | 1.0 (0.99–1.0), 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Važgėlienė, D.; Kubilius, R.; Bileviciute-Ljungar, I. Do Comorbidities and Daily Medication before SARS-CoV-2 Infection Play a Role in Self-Reported Post-Infection Symptoms? J. Clin. Med. 2022, 11, 6278. https://doi.org/10.3390/jcm11216278
Važgėlienė D, Kubilius R, Bileviciute-Ljungar I. Do Comorbidities and Daily Medication before SARS-CoV-2 Infection Play a Role in Self-Reported Post-Infection Symptoms? Journal of Clinical Medicine. 2022; 11(21):6278. https://doi.org/10.3390/jcm11216278
Chicago/Turabian StyleVažgėlienė, Dovilė, Raimondas Kubilius, and Indre Bileviciute-Ljungar. 2022. "Do Comorbidities and Daily Medication before SARS-CoV-2 Infection Play a Role in Self-Reported Post-Infection Symptoms?" Journal of Clinical Medicine 11, no. 21: 6278. https://doi.org/10.3390/jcm11216278
APA StyleVažgėlienė, D., Kubilius, R., & Bileviciute-Ljungar, I. (2022). Do Comorbidities and Daily Medication before SARS-CoV-2 Infection Play a Role in Self-Reported Post-Infection Symptoms? Journal of Clinical Medicine, 11(21), 6278. https://doi.org/10.3390/jcm11216278