
Sustained Hyperglycemia and Its Relationship with the Outcome of Hospitalized Patients with Severe COVID-19: Potential Role of ACE2 Upregulation
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Clinical Information
2.3. Cell Culture and Cell Viability Testing
(A high control) − (A low control)
2.4. RNA Extraction and Complementary DNA (cDNA) Synthesis from A549 Cells
2.5. Measurement of ACE2 Messenger RNA (mRNA) Expression by qRT-PCR
2.6. Statistical Methods
3. Results
3.1. Characteristics of the Study Population
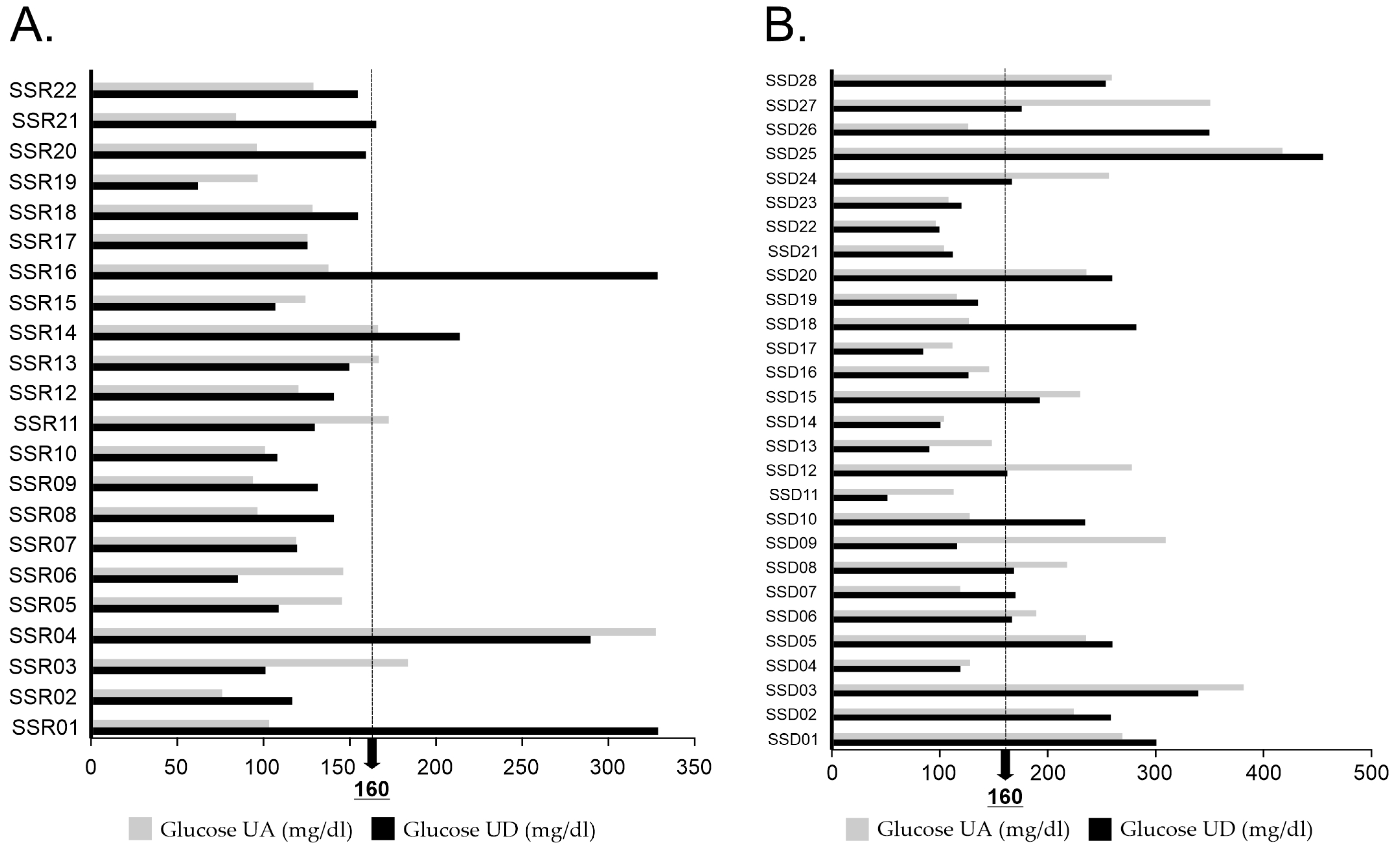
3.2. Clinical and Biochemical Parameters
3.3. High Glucose Treatment Reduced the Viability of A549 Cells
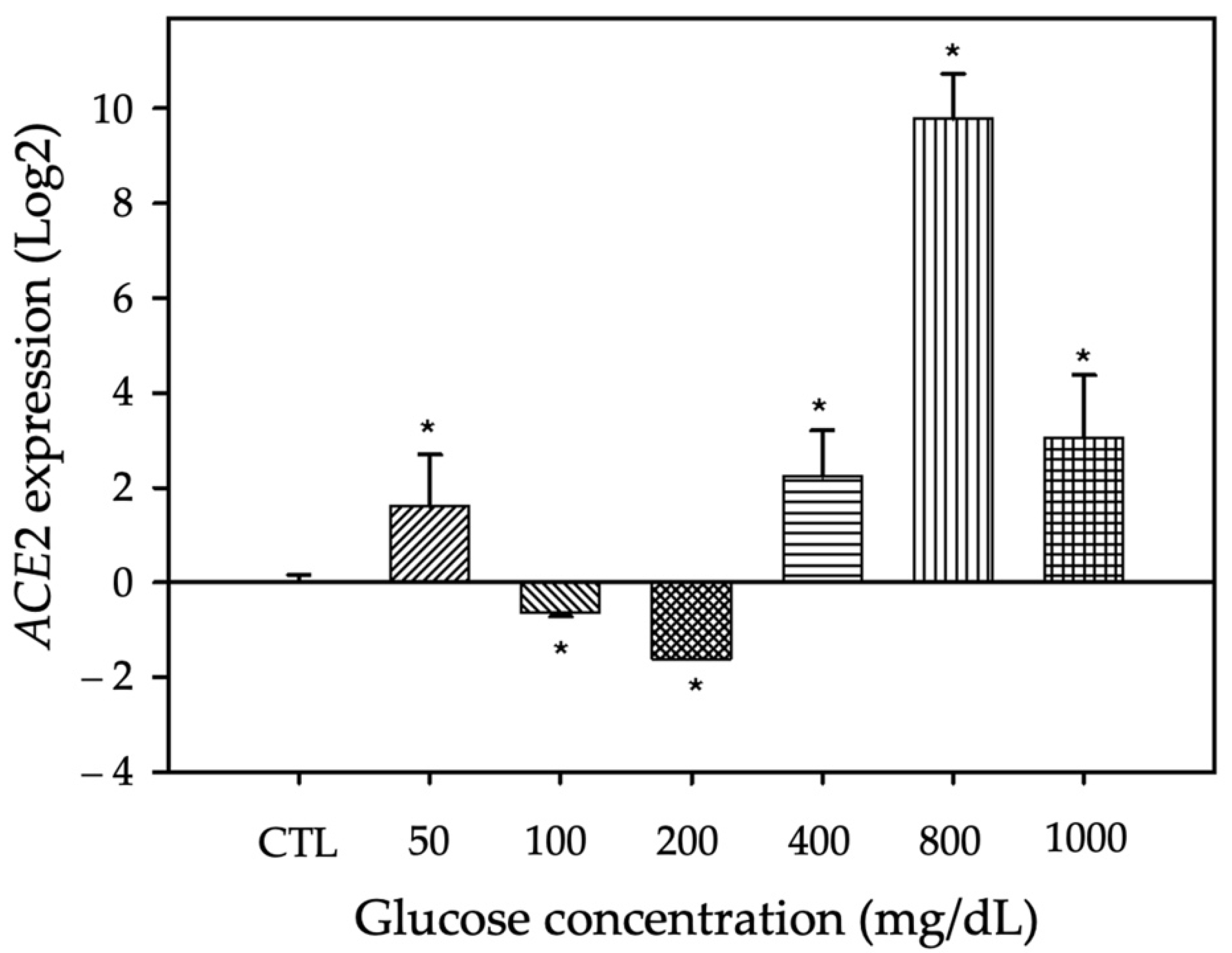
3.4. ACE2 mRNA Expression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hussain, A.; Bhowmik, B.; do Vale Moreira, N.C. COVID-19 and diabetes: Knowledge in progress. Diabetes Res. Clin. Pract. 2020, 162, 108142. [Google Scholar] [CrossRef]
- Medicine, J.H.U. COVID-19 Dashboard. Available online: https://coronavirus.jhu.edu/map.html (accessed on 1 May 2022).
- CONACyT COVID-19 México. Available online: https://coronavirus.gob.mx/datos/ (accessed on 1 May 2022).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Heald, A.H.; Jenkins, D.A.; Williams, R.; Sperrin, M.; Mudaliar, R.N.; Syed, A.; Naseem, A.; Bowden Davies, K.A.; Peng, Y.; Peek, N.; et al. Mortality in People with Type 2 Diabetes Following SARS-CoV-2 Infection: A Population Level Analysis of Potential Risk Factors. Diabetes Ther. 2022, 13, 1037–1051. [Google Scholar] [CrossRef]
- Singh, A.K.; Singh, R. Hyperglycemia without diabetes and new-onset diabetes are both associated with poorer outcomes in COVID-19. Diabetes Res. Clin. Pract. 2020, 167, 108382. [Google Scholar] [CrossRef] [PubMed]
- Lima-Martinez, M.M.; Carrera Boada, C.; Madera-Silva, M.D.; Marin, W.; Contreras, M. COVID-19 and diabetes: A bidirectional relationship. Clin. Investig. Arterioscler. 2021, 33, 151–157. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.K.; Feng, Y.; Yuan, M.Y.; Yuan, S.Y.; Fu, H.J.; Wu, B.Y.; Sun, G.Z.; Yang, G.R.; Zhang, X.L.; Wang, L.; et al. Plasma glucose levels and diabetes are independent predictors for mortality and morbidity in patients with SARS. Diabete Med. 2006, 23, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Badawi, A.; Ryoo, S.G. Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): A systematic review and meta-analysis. Int. J. Infect. Dis. 2016, 49, 129–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Almeida-Pititto, B.; Dualib, P.M.; Zajdenverg, L.; Dantas, J.R.; de Souza, F.D.; Rodacki, M.; Bertoluci, M.C.; Brazilian Diabetes Society Study Group. Severity and mortality of COVID 19 in patients with diabetes, hypertension and cardiovascular disease: A meta-analysis. Diabetol. Metab. Syndr. 2020, 12, 75. [Google Scholar] [CrossRef] [PubMed]
- Gentile, S.; Strollo, F.; Ceriello, A. COVID-19 infection in Italian people with diabetes: Lessons learned for our future (an experience to be used). Diabetes Res. Clin. Pract. 2020, 162, 108137. [Google Scholar] [CrossRef]
- Singh, A.K.; Khunti, K. Assessment of risk, severity, mortality, glycemic control and antidiabetic agents in patients with diabetes and COVID-19: A narrative review. Diabetes Res. Clin. Pract. 2020, 165, 108266. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A.; Hinedi, K.; Ghandour, J.; Khairalla, H.; Musleh, S.; Ujayli, A.; Memish, Z.A. Middle East respiratory syndrome coronavirus: A case-control study of hospitalized patients. Clin. Infect. Dis. 2014, 59, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Akbar, D.H. Bacterial pneumonia: Comparison between diabetics and non-diabetics. Acta Diabetol. 2001, 38, 77–82. [Google Scholar] [CrossRef]
- Iacobellis, G.; Penaherrera, C.A.; Bermudez, L.E.; Bernal Mizrachi, E. Admission hyperglycemia and radiological findings of SARS-CoV2 in patients with and without diabetes. Diabetes Res. Clin. Pract. 2020, 164, 108185. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, C.P.; Oliveira, M.D.; Faro, G.B.; Silva, E.C.; Rocha, E.A.; Barreto-Filho, J.A.; Oliveira, J.L.; Sousa, A.C. Prognostic value of stress hyperglycemia for in-hospital outcome in acute coronary artery disease. Arq. Bras. Cardiol. 2013, 100, 127–134. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marik, P.E.; Bellomo, R. Stress hyperglycemia: An essential survival response! Crit. Care 2013, 17, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.P.; Zhang, Q.; Wang, W.; Zhang, M.; Liu, C.; Xiao, X.; Liu, Z.; Hu, W.M.; Jin, P. Hyperglycemia is a strong predictor of poor prognosis in COVID-19. Diabetes Res. Clin. Pract. 2020, 167, 108338. [Google Scholar] [CrossRef]
- Ceriello, A. Hyperglycemia and the worse prognosis of COVID-19. Why a fast blood glucose control should be mandatory. Diabetes Res. Clin. Pract. 2020, 163, 108186. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Milionis, C.; Milioni, S.O. A brief analysis and hypotheses about the risk of COVID-19 for people with type 1 and type 2 diabetes mellitus. J. Diabetes Metab. Disord. 2020, 19, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef]
- South, A.M.; Diz, D.I.; Chappell, M.C. COVID-19, ACE2, and the cardiovascular consequences. Am. J. Physiol. Heart Circ. Physiol. 2020, 318, H1084–H1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pal, R.; Bhansali, A. COVID-19, diabetes mellitus and ACE2: The conundrum. Diabetes Res. Clin. Pract. 2020, 162, 108132. [Google Scholar] [CrossRef] [PubMed]
- Sartore, G.; Bassani, D.; Ragazzi, E.; Traldi, P.; Lapolla, A.; Moro, S. In silico evaluation of the interaction between ACE2 and SARS-CoV-2 Spike protein in a hyperglycemic environment. Sci. Rep. 2021, 11, 22860. [Google Scholar] [CrossRef]
- D’Onofrio, N.; Scisciola, L.; Sardu, C.; Trotta, M.C.; De Feo, M.; Maiello, C.; Mascolo, P.; De Micco, F.; Turriziani, F.; Municino, E.; et al. Glycated ACE2 receptor in diabetes: Open door for SARS-COV-2 entry in cardiomyocyte. Cardiovasc. Diabetol. 2021, 20, 99. [Google Scholar] [CrossRef]
- Brufsky, A. Hyperglycemia, hydroxychloroquine, and the COVID-19 pandemic. J. Med. Virol. 2020, 92, 770–775. [Google Scholar] [CrossRef] [Green Version]
- Roca-Ho, H.; Riera, M.; Palau, V.; Pascual, J.; Soler, M.J. Characterization of ACE and ACE2 Expression within Different Organs of the NOD Mouse. Int. J. Mol. Sci. 2017, 18, 563. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Zeng, H.; Hao, L.; Zhao, N.; Du, C.; Liao, H.; Wang, Y. Effects of hydroxyapatite microparticle morphology on bone mesenchymal stem cell behavior. J. Mater. Chem. B 2014, 2, 4703–4710. [Google Scholar] [CrossRef]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Rao, X.; Huang, X.; Zhou, Z.; Lin, X. An improvement of the 2^(-delta delta CT) method for quantitative real-time polymerase chain reaction data analysis. Biostat. Bioinform. Biomath. 2013, 3, 71–85. [Google Scholar]
- Panel, I.E. Guía clínica para el tratamiento de la COVID-19 en México. Catálogo Maest. Guías Práct. Clín. 2021, 8, 66. [Google Scholar]
- American Diabetes Association. 15. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S211–S220. [Google Scholar] [CrossRef] [PubMed]
- Tonon, F.; Candido, R.; Toffoli, B.; Tommasi, E.; Cortello, T.; Fabris, B.; Bernardi, S. Type 1 diabetes is associated with significant changes of ACE and ACE2 expression in peripheral blood mononuclear cells. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Saand, A.R.; Flores, M.; Kewan, T.; Alqaisi, S.; Alwakeel, M.; Griffiths, L.; Wang, X.; Han, X.; Burton, R.; Al-Jaghbeer, M.J.; et al. Does inpatient hyperglycemia predict a worse outcome in COVID-19 intensive care unit patients? J. Diabetes 2021, 13, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Azar, W.S.; Njeim, R.; Fares, A.H.; Azar, N.S.; Azar, S.T.; El Sayed, M.; Eid, A.A. COVID-19 and diabetes mellitus: How one pandemic worsens the other. Rev. Endocr. Metab. Disord. 2020, 21, 451–463. [Google Scholar] [CrossRef]
- Albulescu, R.; Dima, S.O.; Florea, I.R.; Lixandru, D.; Serban, A.M.; Aspritoiu, V.M.; Tanase, C.; Popescu, I.; Ferber, S. COVID-19 and diabetes mellitus: Unraveling the hypotheses that worsen the prognosis (Review). Exp. Ther. Med. 2020, 20, 194. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Bhadada, S.K. COVID-19 and diabetes mellitus: An unholy interaction of two pandemics. Diabetes Metab. Syndr. 2020, 14, 513–517. [Google Scholar] [CrossRef]
- Huang, X.; Dong, W.; Milewska, A.; Golda, A.; Qi, Y.; Zhu, Q.K.; Marasco, W.A.; Baric, R.S.; Sims, A.C.; Pyrc, K.; et al. Human Coronavirus HKU1 Spike Protein Uses O-Acetylated Sialic Acid as an Attachment Receptor Determinant and Employs Hemagglutinin-Esterase Protein as a Receptor-Destroying Enzyme. J. Virol. 2015, 89, 7202–7213. [Google Scholar] [CrossRef] [Green Version]
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. China CDC Wkly. 2020, 41, 145–151. [Google Scholar]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Docherty, A.B.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; Merson, L.; et al. Malcolm Gracie Semple. Features of 16,749 hospitalised UK patients with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol. Medrxiv Prepr. 2020, 04, 23. [Google Scholar]
- Bello-Chavolla, O.Y.; Bahena-Lopez, J.P.; Antonio-Villa, N.E.; Vargas-Vazquez, A.; Gonzalez-Diaz, A.; Marquez-Salinas, A.; Fermin-Martinez, C.A.; Naveja, J.J.; Aguilar-Salinas, C.A. Predicting Mortality Due to SARS-CoV-2: A Mechanistic Score Relating Obesity and Diabetes to COVID-19 Outcomes in Mexico. J. Clin. Endocrinol. Metab. 2020, 105, 2752–2761. [Google Scholar] [CrossRef]
- Hulme, K.D.; Gallo, L.A.; Short, K.R. Influenza Virus and Glycemic Variability in Diabetes: A Killer Combination? Front. Microbiol. 2017, 8, 861. [Google Scholar] [CrossRef] [PubMed]
- George, C.; Ducatman, A.M.; Conway, B.N. Increased risk of respiratory diseases in adults with Type 1 and Type 2 diabetes. Diabetes Res. Clin. Pract. 2018, 142, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Delamaire, M.; Maugendre, D.; Moreno, M.; Le Goff, M.C.; Allannic, H.; Genetet, B. Impaired leucocyte functions in diabetic patients. Diabetes Med. 1997, 14, 29–34. [Google Scholar] [CrossRef]
- Sardu, C.; Marfella, R.; Prattichizzo, F.; La Grotta, R.; Paolisso, G.; Ceriello, A. Effect of Hyperglycemia on COVID-19 Outcomes: Vaccination Efficacy, Disease Severity, and Molecular Mechanisms. J. Clin. Med. 2022, 11, 1564. [Google Scholar] [CrossRef]
- Prasad, K.; Mishra, M. Do Advanced Glycation End Products and Its Receptor Play a Role in Pathophysiology of Hypertension? Int. J. Angiol. 2017, 26, 1–11. [Google Scholar]
- Machahua, C.; Montes-Worboys, A.; Llatjos, R.; Escobar, I.; Dorca, J.; Molina-Molina, M.; Vicens-Zygmunt, V. Increased AGE-RAGE ratio in idiopathic pulmonary fibrosis. Respir. Res. 2016, 17, 144. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | COVID-19 Outcome (n = 50) | p-Value | OR (95% CI) | |
|---|---|---|---|---|
| Death (n = 28) | Recovery (n = 22) | |||
| Sex n (%) | ||||
| Male | 9 (42.9) | 12 (57.1) | 0.616 | - |
| Female | 19 (65.5) | 10 (34.5) | ||
| Age (years) | 59.4 ± 14.1 | 55.9 ± 13.9 | <0.001 * | - |
| Hospital Stay (days) | 21 ± 18 | 10 ± 8 | 0.004 * | |
| Symptoms n (%) | ||||
| Fever | 9 (32.1) | 10 (45.5) | 0.503 | 0.6 (0.2–1.8) |
| Cough | 8 (28.6) | 12 (54.5) | 0.116 | 0.3 (0.1–1.1) |
| Cefalea | 6 (21.4) | 9 (40.9) | 0.238 | 0.4 (1.1–1.4) |
| Dyspnea | 13 (46.4) | 14 (63.6) | 0.354 | 0.5 (0.2–1.6) |
| Tachypnea | 13 (46.4) | 12 (54.5) | 0.776 | 0.7 (0.2–2.2) |
| Tachycardia | 3 (10.7) | 2 (9.1) | 1 | 1.2 (0.2–7.9) |
| Chest pain | 2 (7.1) | 2 (9.1) | 1 | 0.7 (0.1–5.9) |
| Diarrhea | 4 (14.3) | 1 (4.5) | 0.368 | 3.5 (0.4–33.8) |
| Asthenia | 6 (21.4) | 5 (22.7) | 1 | 0.9 (0.2–3.6) |
| Adynamia | 6 (21.4) | 5 (22.7) | 1 | 0.9 (0.2–3.6) |
| Myalgia | 3 (10.7) | 7 (31.8) | 0.084 | 0.3 (0.06–1.1) |
| Arthralgia | 2 (7.1) | 7 (31.8) | 0.032 * | 0.2 (0.03–0.9) |
| Anosmia | 0 (0) | 2 (9.1) | 0.189 | ---- |
| Dysgeusia | 0 (0) | 4 (18.2) | 0.032 * | ---- |
| Odynophagia | 2 (7.1) | 1 (4.5) | 1 | 1.6 (0.1–19.1) |
| General discomfort | 3 (10.7) | 2 (9.1) | 1 | 1.2 (0.2–7.9) |
| Rhinorrhea | 4 (14.3) | 2 (9.1) | 0.638 | 1.7 (0.3–10.1) |
| Variable n (%) | COVID-19 Outcome (n = 50) | p-Value | OR (95% CI) | |
|---|---|---|---|---|
| Death (n = 28) | Recovery (n = 22) | |||
| Arterial hypertension | 18 (64.3) | 6 (27.3) | 0.021 * | 4.8 (1.4–16.2) |
| Obesity | 6 (21.4) | 2 (9.1) | 0.439 | 2.3 (0.5–15.1) |
| Diabetes mellitus | 10 (35.7) | 5 (22.7) | 0.494 | 1.9 (0.5–6.7) |
| Stress hyperglycemia | 17 (60.7) | 15 (68.2) | 0.803 | 0.7 (0.2–2.3) |
| Supplemental oxygen | 28 (100) | 18 (81.8) | 0.032 * | ---- |
| Over-aggregated pneumonia | 6 (21.4) | 1 (4.5) | 0.117 | 5.7 (0.6–51.7) |
| Mechanical ventilation | 22 (78.6) | 2 (9.1) | <0.001 * | 36.7 (6.6–202.9) |
| HG > 160 mg/dl UA | 14 (50) | 6 (27.3) | 0.181 | 2.7 (0.8–8.8) |
| HG > 160 mg/dl UD | 17 (60.7) | 5 (22.7) | 0.016 * | 5.3 (1.5–18.4) |
| Glucose Concentration | Time (hours) | p-Value | ||
|---|---|---|---|---|
| 24 | 48 | 72 | ||
| Control | −1.568 ± 1.872 | −1.568 ± 1.872 | −1.568 ± 1.872 | ----- |
| 50 mg/dl | 2.175 ±0.00175 | −0.0322 ± 0.838 | 1.734 ± 0.614 | 0.067 |
| 100 mg/dl | 0.891 ± 0.825 | 0.467 ± 0.378 | −0.43 ± 0.204 | 0.138 |
| 200 mg/dl | 0.234 ± 0.0589 | 1.193 ± 0.644 | −1.473 ± 0.608 | 0.03 * |
| 400 mg/dl | 0.698 ± 0.704 | −1.178 ± 0.204 | 2.375 ± 0.922 | 0.031 * |
| 800 mg/dl | 0.717 ± 0.00902 | −0.672 ± 0.129 | 9.91 ± 1.312 | 0.001 * |
| 1000 mg/dl | −0.658 ± 1.346 | 1.13 ± 2.048 | 3.172 ± 2.339 | 0.29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vargas-Rodriguez, J.R.; Valdés Aguayo, J.J.; Garza-Veloz, I.; Martinez-Rendon, J.; del Refugio Rocha Pizaña, M.; Cabral-Pacheco, G.A.; Juárez-Alcalá, V.; Martinez-Fierro, M.L. Sustained Hyperglycemia and Its Relationship with the Outcome of Hospitalized Patients with Severe COVID-19: Potential Role of ACE2 Upregulation. J. Pers. Med. 2022, 12, 805. https://doi.org/10.3390/jpm12050805
Vargas-Rodriguez JR, Valdés Aguayo JJ, Garza-Veloz I, Martinez-Rendon J, del Refugio Rocha Pizaña M, Cabral-Pacheco GA, Juárez-Alcalá V, Martinez-Fierro ML. Sustained Hyperglycemia and Its Relationship with the Outcome of Hospitalized Patients with Severe COVID-19: Potential Role of ACE2 Upregulation. Journal of Personalized Medicine. 2022; 12(5):805. https://doi.org/10.3390/jpm12050805
Chicago/Turabian StyleVargas-Rodriguez, Jose R., José J. Valdés Aguayo, Idalia Garza-Veloz, Jacqueline Martinez-Rendon, Maria del Refugio Rocha Pizaña, Griselda A. Cabral-Pacheco, Vladimir Juárez-Alcalá, and Margarita L. Martinez-Fierro. 2022. "Sustained Hyperglycemia and Its Relationship with the Outcome of Hospitalized Patients with Severe COVID-19: Potential Role of ACE2 Upregulation" Journal of Personalized Medicine 12, no. 5: 805. https://doi.org/10.3390/jpm12050805