
COVID-19 Pandemical Period: Issues and Strategies to Make Sustainable Socialization and Recreation for Elderly People in Long-Term Care Institutions


Abstract
:1. Introduction
2. Theoretical Background
2.1. The Long-Term Care Institutions
2.2. The Industry 4.0 and Healthcare
3. Materials and Methods
The Empirical Research
4. Results and Discussions
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
References
- Brazilian Institute of Geography and Statistics (IBGE). Pesquisa Nacional De Saneamento Básico Brasil; Brazilian Institute of Geography and Statistics (IBGE): Rio de Janeiro, Brazil, 2019. Available online: https://censo2020.ibge.gov.br/2012-agencia-de-noticias/noticias/24036-idosos-indicam-caminhos-para-uma-melhor-idade.html#:~:text=De%20acordo%20com%20a%20Organiza%C3%A7%C3%A3o,13%25%20da%20popula%C3%A7%C3%A3o%20do%20pa%C3%ADs (accessed on 23 August 2022).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Do IBGE Revela Que Aumentou o Número de Usuários de Internet no Brasil; Brazilian Institute of Geography and Statistics, IBGE: Rio de Janeiro, Brazil, 2018. Available online: https://canaltech.com.br/internet/pesquisa-do-ibge-revela-que-aumentou-o-numero-de-usuarios-de-internet-no-brasil-129545/ (accessed on 23 August 2022).
- ANVISA. Resolução de Diretoria Colegiada—RDC No. 283. Available online: http://portal.anvisa.gov.br/documents/10181/2718376/RDC_283_2005_COMP.pdf/a38f2055-c23a-4eca-94ed-76fa43acb1df (accessed on 29 December 2021).
- Garrido, R.; Menezes, P.R. O Brasil está envelhecendo: Boas e más notícias por uma perspectiva epidemiológica. Rev. Bras. Psiquiatr. 2002, 24, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Fagundes, V.D.L.; Esteves, K.R.; Ribeiro, M.M.; Siepierski, J.H.; Da Silva, C.T.; Vitor, J.; Mendes, M.A. Instituições de longa permanência como alternativa no acolhimento das pessoas idosas. Rev. Salud Pública 2017, 19, 210–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portal da Cidade de São Paulo. Serviço para Cidadão. Available online: http://www.capital.sp.gov.br/cidadao/familia-e-assistencia-social/centros-de-acolhida/centros-de-acolhida-espLTCal/instituicao-de-longa-permanencia-para-idoso-ilpi (accessed on 29 December 2021).
- ACASA. O Papel Das Instituições de Longa Permanência Para Idosos. 2020. Available online: https://www.grupoacasa.com.br/ilpi/ (accessed on 29 December 2021).
- Camarano, A.A.; Kanso, S. As instituições de longa permanência para idosos no Brasil. Rev. Bras. Estud. Popul. 2010, 27, 1. [Google Scholar] [CrossRef] [Green Version]
- Creutzberg, M.; Gonçalves, L.H.T.; Sobottka, E.A.; Ojeda, B.S. A instituição de longa permanência para idosos e o sistema de saúde. Rev. Lat. Am. Enferm. 2007, 15, 6. [Google Scholar]
- Abbasi, J. Social Isolation—The Other COVID-19 Threat in Nursing Homes. JAMA 2020, 324, 7. [Google Scholar] [CrossRef]
- Scheffers, F.; Moonen, X.; van Vugt, E. Assessing the quality of support and discovering sources of resilience during COVID-19 measures in people with intellectual disabilities by professional carers. Res. Dev. Disabil. 2021, 111, 103889. [Google Scholar] [CrossRef]
- Miyah, Y.; Benjelloun, M.; Lairini, S.; Lahrichi, A. COVID-19 Impact on Public Health, Environment, Human Psychology, Global Socioeconomy, and Education Hindawi. Sci. World J. 2022, 2022, 8. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, U. Disparate impact pandemic framing decreases public concern for health consequences. PLoS ONE 2020, 15, e0243599. [Google Scholar] [CrossRef]
- Jeong, S.-A.; Kim, J. Factors influencing nurses’ intention to care for patients with COVID-19: Focusing on positive psychological capital and nursing professionalism. PLoS ONE 2022, 17, e0262786. [Google Scholar] [CrossRef]
- Zhang, H.H.; Zhao, Y.J.; Wang, C.; Zhang, Q.; Yu, H.Y.; Cheung, T.; Hall, B.J.; An, F.R.; Xiang, Y.T. Depression, and its relationship with quality of life in frontline psychiatric clinicians during the COVID-19 pandemic in China: A national survey. Int. J. Biol. Sci. 2021, 17, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.; Scavarda, A.; Reis, A.; Silveira, H.; Ebecken, N.F.F. Managerial Strategies for Elderly care Organization Professionals: COVID-19 Pandemic Impacts. Sustainability 2020, 12, 9682. [Google Scholar] [CrossRef]
- Charlene, H.; Chu, S.D.W.; Christopher, J.D. Competing crises: COVID-19 countermeasures and social isolation among older adults in elderly care. J. Adv. Nurs. 2020, 76, 2456–2459. [Google Scholar]
- VanderWeele, T.J. Challenges Estimating Total Lives Lost in COVID-19 DLTCsions Consideration of Mortality Related to Unemployment, Social Isolation, and Depression. JAMA 2020, 324, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Office, E.E.; Rodenstein, M.S.; Merchant, T.S.; Pendergrast, T.R.; Lindquist, L.A. Reducing Social Isolation of Seniors during COVID-19 through Medical Student Telephone Contact. J. Am. Med. Dir. Assoc. 2020, 21, 948–950. [Google Scholar] [CrossRef]
- Di Fazio, N.; Caporale, M.; Fazio, V.; Delogu, G.; Frati, P. Italian law no. 1/2021 on the subject of vaccination against Covid-19 in people with mental disabilities within the nursing homes. Clin. Ther. 2021, 172, 414–419. [Google Scholar] [CrossRef]
- De Lima, A.G.; Pinto, G.S. Industry 4.0: A new paradigm for industry. Interface Tecnol. 2019, 16, 299–311. [Google Scholar] [CrossRef] [Green Version]
- Kusma, V.V.; Chiroli, D.M.d.G. A indústria 4.0: Uma revisão sobre os impactos e as modificações na dinâmica de trabalho do modelo atual. Rev. Principia 2021, 1, 131–140. [Google Scholar] [CrossRef]
- Palma, J.M.B.; Bueno, U.S.; Storolli, W.G.; Schiavuzzo, P.L.; Cesar, F.I.G.; Makiya, I.K. Os princípios da Indústria 4.0 e os impactos na sustentabilidade da cadeia de valor empresarial. In Proceedings of the 6th International Workshop Advances in Cleaner Production 2017, Sao Paulo, Brazil, 24–26 May 2017. [Google Scholar]
- Julianelli, V.; Caiado, R.G.G.; Scavarda, L.F.; Cruz, S.P.d.M.F. Interplay between reverse logistics and circular economy: Critical success factors-based taxonomy and framework. Resour. Conserv. Recycl. 2020, 158, 104784. [Google Scholar] [CrossRef]
- Santos, A.; Macedo, J.; Costa, A.M.; Nicolau, J. Internet of Things and Smart Objects for M-Health Monitoring and Control. Procedia Technol. 2014, 16, 1351–1360. [Google Scholar] [CrossRef] [Green Version]
- Laplante, P.A.; Laplante, N. The Internet of Things in Healthcare Potential Applications and Challenges. IEEE Comput. Soc. 2016, 18, 2–4. [Google Scholar] [CrossRef]
- Wolf, B.; Scholze, C. Medicine 4.0, the Importance of Electronics, Information Technology and Microsystems in Modern Medicine—The Case of Customized Chemotherapy. Curr. Dir. Biomed. Eng. 2017, 34, 183–186. [Google Scholar] [CrossRef]
- Mariano, A.S.; Souza, N.M.; Cavaco, A.; Lopes, L.C. Healthcare professionals’ behavior, skills, knowledge, and attitudes on evidence-based health practice: A protocol of cross-sectional study. BMJ Open 2018, 8, 6. [Google Scholar] [CrossRef] [PubMed]
- Kumari, A.; Tanwar, S.; Tyagi, S.; Kumar, N. Fog computing for healthcare 4.0 environment: Opportunities and challenges. Comput. Electr. Eng. 2018, 72, 1–13. [Google Scholar] [CrossRef]
- Dau, G.; Scavarda, A.; Scavarda, L.F.; Portugal, V.J.T. The Healthcare Sustainable Supply Chain 4.0: The Circular Economy Transition Conceptual Framework with the Corporate Social Responsibility Mirror. Sustainability 2019, 11, 3259. [Google Scholar] [CrossRef] [Green Version]
- Javaid, M.; Haleem, A.; Vaishya, R.; Bahl, S.; Suman, R.; Vaish, A. Industry 4.0 technologies and their applications in fighting COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 419–422. [Google Scholar] [CrossRef]
- Arthur-Holmes, F.; Akaadom, M.K.A.; Agyemang-Duah, W.; Abrefa Busia, K.; Peprah, P. Healthcare Concerns of Older Adults during the COVID-19 Outbreak in Low- and Middle-Income Countries: Lessons for Health Policy and Social Work. J. Gerontol. Soc. Work. 2020, 63, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Aceto, G.; Persico, V.; Pescape, A. Industry 4.0 and Health: Internet of Things, Big Data, and Cloud Computing for Healthcare 4.0. J. Ind. Inf. Integr. 2020, 18, 100129. [Google Scholar] [CrossRef]
- Caceres, C.; Rosario, J.M.; Amaya, D. Towards Health 4.0: E-Hospital Proposal Based Industry 4.0 and Artificial Intelligence Concepts. Artif. Intell. Med. 2019, 11526, 84–89. [Google Scholar] [CrossRef]
- Branger, J.; Pang, Z. From automated home to sustainable, healthy, and manufacturing home: A new story enabled by the Internet-of-Things and Industry 4.0. J. Manag. Anal. 2015, 2, 314–332. [Google Scholar] [CrossRef]
- Scavarda, A.; Dau, G.; Scavarda, L.F.; Azevedo, B.D.; Korzenowski, A.L. Social and ecological approaches in urban interfaces: A sharing economy management Framework. Sci. Total Environ. 2019, 713, 134407. [Google Scholar] [CrossRef] [PubMed]
- Elhoseny, M.; Abdelaziz, A.; Salama, A.S.; Riad, A.M.; Muhammade, K.; Sangaiah, A.K. A hybrid model of Internet of Things and cloud computing to manage big data in health services applications. Future Gener. Comput. Syst. 2018, 86, 1383–1394. [Google Scholar] [CrossRef]
- Graham, C.M.; Jones, N. Impact of IoT on geriatric telehealth. Work. Older People 2020, 24, 231–243. [Google Scholar] [CrossRef]
- Monteiro, A.C.B.; França, R.P.; Estrela, V.V.; Iano, Y.; Khelassi, A.; Razmjooy, N. Health 4.0: Applications, Management, Technologies, and Review. Med. Technol. J. 2018, 2, 262–276. [Google Scholar] [CrossRef]
- Rocha, T.A.H.; Fachini, L.A.; Thume, E.; da Silva, N.C.; Barbosa, A.C.Q.; Carmo, M.d.J.; Rodrigues, M. Mobile health: New perspectives for healthcare provision. Epidemiol. Serv. Saude 2016, 25, 159–170. [Google Scholar] [CrossRef]
- Dias, A.C.; Reis, A.C.; Oliveira, R.P.; Maruyama, U.G.R.; Martinez, P. Lean Manufacturing in Healthcare: A Systematic Review of Literature. Rev. Produção E Desenvolv. 2018, 4, 111–122. [Google Scholar] [CrossRef]
- Scavarda, A.; Dias, A.; Reis, A.; Silveira, H.; Santos, I. A COVID-19 Pandemic Sustainable Educational Innovation Management Proposal Framework. Sustainability 2021, 13, 6391. [Google Scholar] [CrossRef]
- Arcidiacono, G.; Pieroni, A. The Revolution Lean Six Sigma 4.0. Int. J. Adv. Sci. Eng. Inf. Technol. 2018, 8, 141–149. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, F.S.; Scavarda, A.; Sellitto, M.A.; Marques, D.I.L. Sustainability in the winemaking industry: An analysis of Southern Brazilian companies based on a literature review. J. Clean. Prod. 2019, 192, 80–87. [Google Scholar] [CrossRef]
- Dias, A.; Scavarda, A.; Silveira, H.; Scavarda, L.F.; Kondamareddy, K.K. The Online Education System: COVID-19 Demands, Trends, Implications, Challenges, Lessons, Insights, Opportunities, Outlooks, and Directions in the Work from Home. Sustainability 2021, 13, 12197. [Google Scholar] [CrossRef]
- Azevedo, B.D.; Scavarda, L.F.; Caiado, R.G.G. Urban solid waste management in developing countries from the sustainable supply chain management perspective: A case study of Brazil’s largest slum. J. Clean. Prod. 2019, 233, 1377–1386. [Google Scholar] [CrossRef]
- Dias, A.; Scavarda, A.; Reis, A.; Silveira, H.; Scavarda, A. Equity, Justice, and Quality during the COVID-19 Pandemic Period: Considerations on Learning and Scholarly Performance in Brazilian Schools. Educ. Sci. 2022, 12, 354. [Google Scholar] [CrossRef]
- Dias, A.C.; Reis, A.C. Estágio Supervisionado em arquivologia: Pontos fortes e fracos e sugestões para de melhoria para o programa. Ciência Inf. 2017, 46, 84–105. [Google Scholar] [CrossRef]
- Sapoval, M.; Gaultier, A.; Del Giudice, C.; Pellerin, O.; Kassis-Chikhani, N.; Lemarteleur, V.; Fouquet, V.; Tapie, L.; Morenton, P.; Tavitian, B.; et al. 3D-printed face protective shield in interventional radiology: Evaluation of an immediate solution in the era of COVID-19 pandemic. Diagn. Interv. Imaging 2020, 101, 413–415. [Google Scholar] [CrossRef]
- Zhong, H.; Zhu, Z.; Lin, J.; Cheung, C.F.; Lu, V.L.; Yan, F.; Chan, C.Y.; Li, G. Reusable and Recyclable Graphene Masks with Outstanding Superhydrophobic and Photothermal Performances. ACS NANO 2020, 15, 6213–6221. [Google Scholar] [CrossRef]
- Smith, A.C.; Thomas, E.; Snoswell, C.L.; Haydon, H.; Mehrotra, A.; Clemensen, J.; Caffery, L.J. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J. Telemed. Telecare 2020, 26, 309–313. [Google Scholar] [CrossRef] [Green Version]
- Belzunegui-Eraso, A.; Erro-Garcés, A. Teleworking in the Context of the COVID-19 Crisis. Sustainability 2020, 12, 3662. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Surveillance Case Definitions for Human Infection with Novel Coronavirus (nCoV); WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/who-documents-detail/surveillance-case-definitions-for-human-infection-withnovel-coronavirus-(ncov) (accessed on 29 December 2021).
- World Health Organization (WHO). Global Surveillance for COVID-19 Caused by Human Infection with COVID-19 Virus; WHO: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/331506/WHO-2019-nCoV-SurveillanceGuidance-2020.6-eng.pdf (accessed on 29 December 2021).
- Giacomin, K.C. Frente Nacional de Fortalecimento às Instituições de Longa Permanência para Idosos; Ministério da Saúde: Brasília, Brazil, 2020. Available online: https://coronavirus.saude.gov.br/sobre-a-doenca#o-que-e-covid (accessed on 29 December 2021).
- Sales, A.E.; Estabrooks, C.A.; Valente, T.W. The impact of social networks on knowledge transfer in elderly care facilities. Implement. Sci. 2010, 5, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockcontent. O Guia Complete de Redes Sociais: Saiba Tudo Sobre as Plataformas de Mídias Sociais! 2020. Available online: https://rockcontent.com/blog/tudo-sobre-redes-sociais/ (accessed on 29 December 2021).
- Universidade Aberta da Terceira Idade (UNATI). Relação Das Instituições de Longa Permanência Para Idosos Do Município Do Rio de Janeiro; UNATI: Punjab, India, 2005; Available online: http://www.unatiuerj.com.br/relacao.pdf (accessed on 29 December 2021).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Minimum | Maximum | Median | Mean | Standard Deviation | Sum | Coefficient Variation |
|---|---|---|---|---|---|---|---|
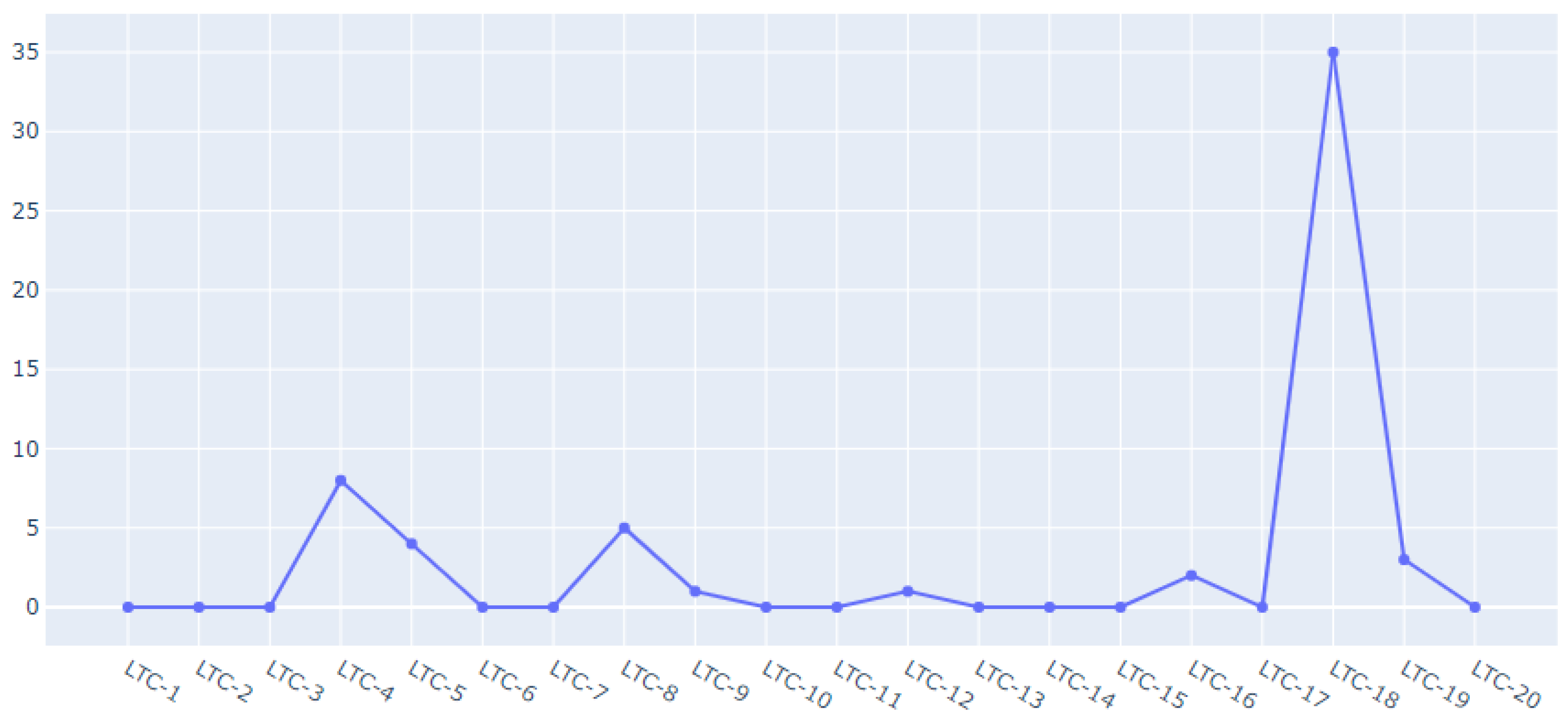
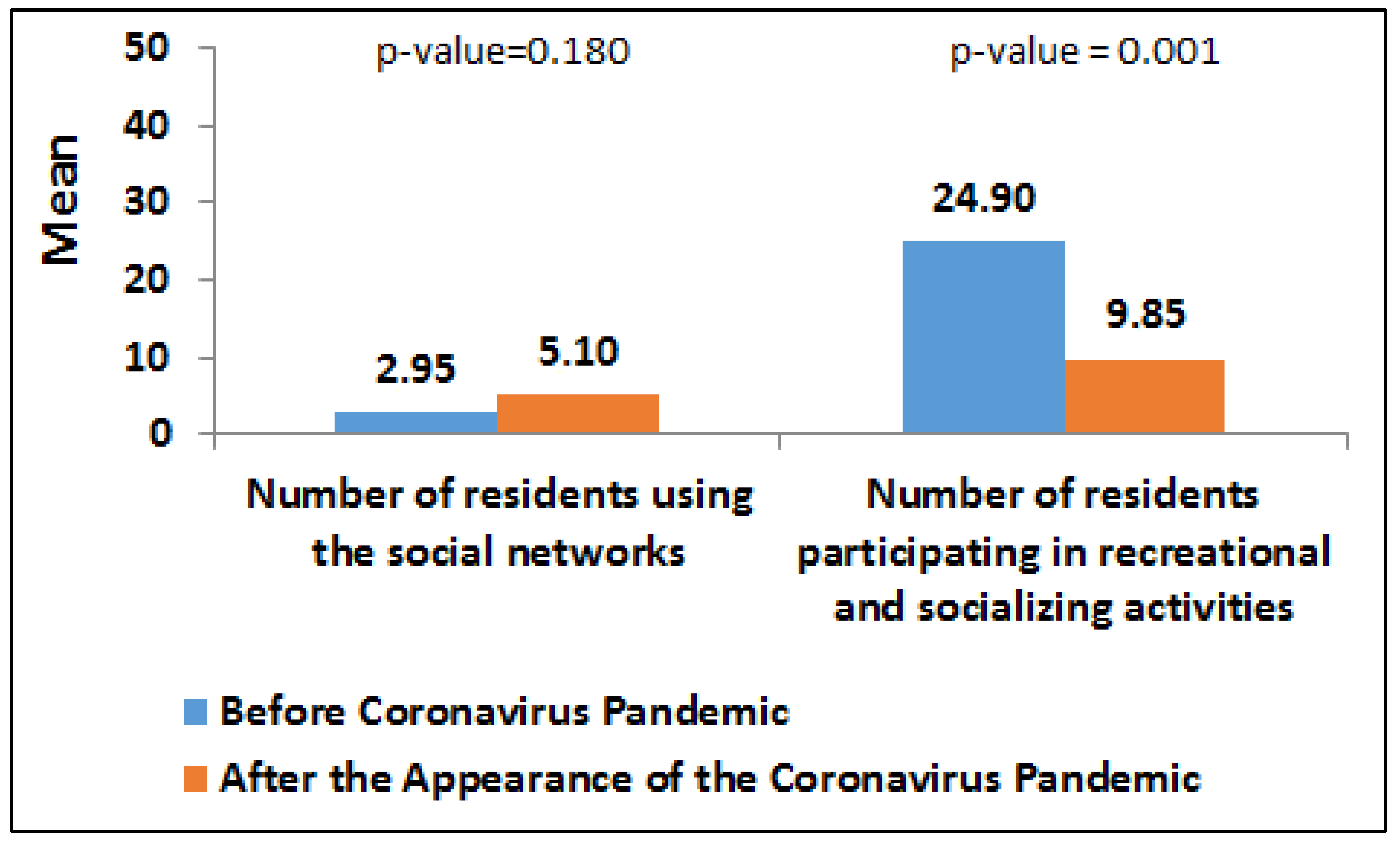
| The number of residents using the social networks before Coronavirus | 0 | 35 | 0.0 | 2.95 | 7.85 | 59 | 2.66 |
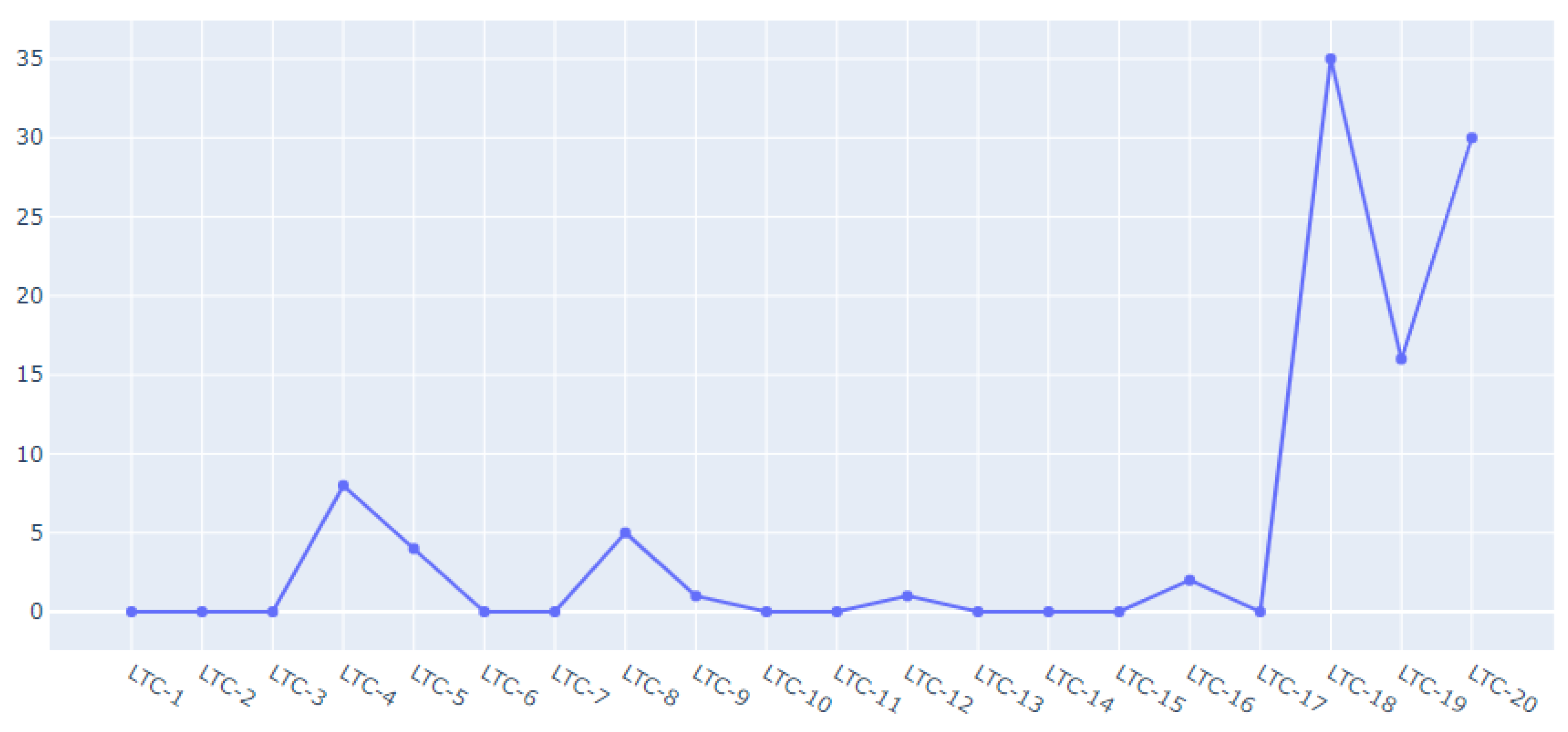
| The number of residents using the social networks after the appearance of the Coronavirus pandemic | 0 | 35 | 0.0 | 5.10 | 10.19 | 102 | 2.00 |
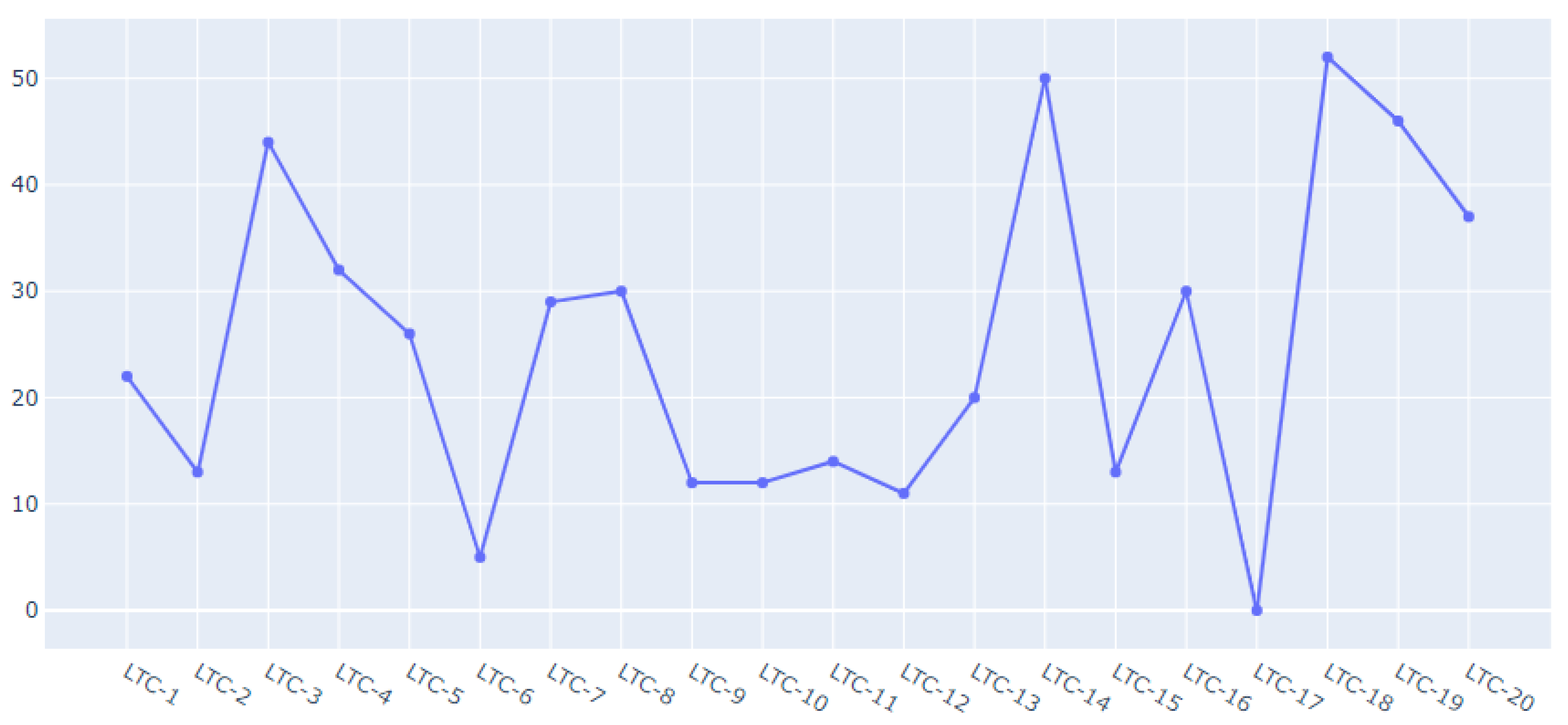
| The number of residents participating in recreational and socializing activities before the Coronavirus pandemic | 0 | 52 | 24.0 | 24.90 | 15.25 | 498 | 0.61 |
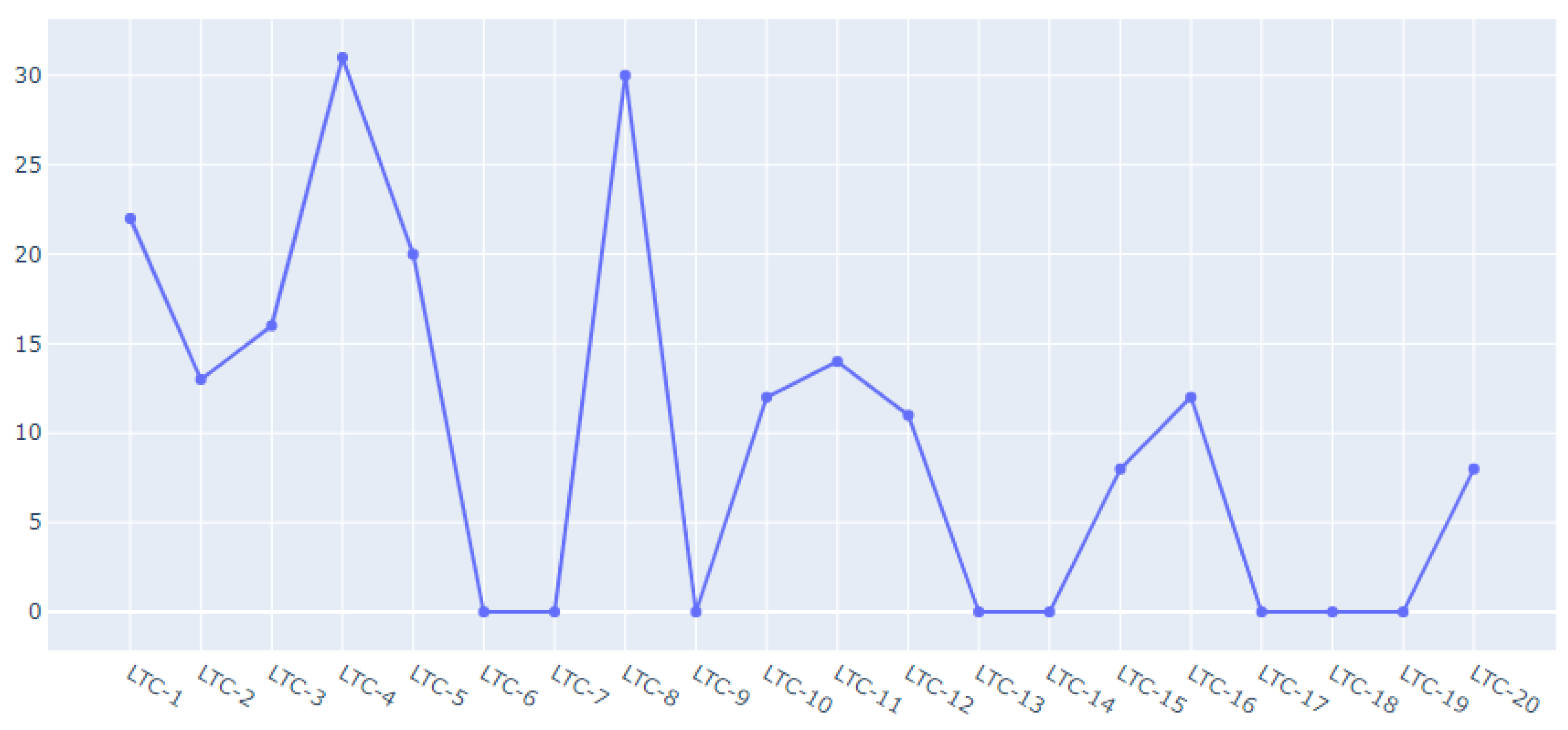
| The number of residents participating in recreational and socializing activities after the appearance of the Coronavirus pandemic | 0 | 31 | 9.5 | 9.85 | 10.16 | 197 | 1.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dias, A.; Scavarda, A.; da Cunha Reis, A.; Santos, I.; Fonseca, A. COVID-19 Pandemical Period: Issues and Strategies to Make Sustainable Socialization and Recreation for Elderly People in Long-Term Care Institutions. COVID 2023, 3, 392-404. https://doi.org/10.3390/covid3030029
Dias A, Scavarda A, da Cunha Reis A, Santos I, Fonseca A. COVID-19 Pandemical Period: Issues and Strategies to Make Sustainable Socialization and Recreation for Elderly People in Long-Term Care Institutions. COVID. 2023; 3(3):392-404. https://doi.org/10.3390/covid3030029
Chicago/Turabian StyleDias, Ana, Annibal Scavarda, Augusto da Cunha Reis, Isabel Santos, and Andre Fonseca. 2023. "COVID-19 Pandemical Period: Issues and Strategies to Make Sustainable Socialization and Recreation for Elderly People in Long-Term Care Institutions" COVID 3, no. 3: 392-404. https://doi.org/10.3390/covid3030029